PSV(Pressure Support Ventilation)
PSV is Siemens Servo It was loaded into 900 C, being the first time.
It is the result of the anguish in the Siemens Elema Inc. development group which persisted in the demand flow method.
To do in the behind of the time gas is actually supplied to which after making a demand flow method the air current resistance of breathing circuit at the trigger compared with the continuous flow method increases an intake work volume.
PSV was contrived as the "pressurizing intake at the constant pressure and offsetting circuit resistance, and applying a little higher pressure and reducing an intake work volume" assisted-ventilation law to solve this.
At present, PSV is high as the ventilation law which helps a spontaneous-respiration or the weaning ventilation law from the resuscitator and is evaluative.
The characteristic of PSV is that all such as the intake time, the intake flow rate, the expiration time, the taking air quantity of ventilation, breathing number of times is fixed in the free will of the patient and the operator can set only PSV pressure and a trigger level.
ü@
(Reference 1) Old and new PSV
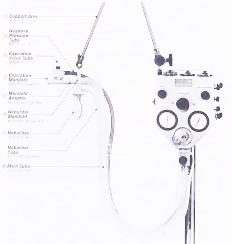
PSV existed already in the early stages of the 1960s.
Then, the new Mattick circuit (Pneumatic circuit) method got evaluation by the good trigger mechanism of the replying and the machine which can be trusted.
This circuit is "the mechanism" which switches a valve and a switch only using the pressure of gas.
The inspiratory-phase was the Pressure limit type (the Å]ł│ type) (classified into Pressure cycle at present) which ends when the airway pressure rises in the set value.
The typical manufacturer includes Bird Inc. and Benette Inc..
PR-2 of the Benette Inc. is classified with the pressure-cycled-respirator which is the same as the Bird series but the operating principle of both is different.
In PR-2, the standing-up of the inspiratory-pressure is early comparatively and the airway pressure reaches a set-pressure in the early stages of the inspiratory-phase (It is merely pressure cycle if intake ends here).
Therefore, this pressure is maintained for a while and the intake current velocity attenuates.
If the intake current velocity becomes below setting current velocity (terminal flow), intake ends (There is this setting knob, that the main unit is to the right).
Also, it has the time cycle mechanism which limits intake time so as not for intake to continue unnecessarily, too.
This is the operating principle which is the same as present PSV completely.
ü@
(Reference 2) The mode of the
similarity of PSV
In the Drager Inc., it is called ASB, in the Engstrom Inc., it is called Inspiration Assistence but these are almost the same operating principle.
ü@
2. The component
PSV is composed of the following three elements.
(1)
The recognition of intake : It (Patient initiated)s an airway pressure decline by the intake effort of the patient with the trigger and æŚŗC starts.
(2)
The inspiratory-phase : It pressurizes the pressure (the PS pressure) to have set the respiratory tract to (Pressure controlled or Pressure regulated).
(3)
The recognition of the ending of intake : It recognizes that the intake current velocity declines and it stops the respiratory tract pressurization and it opens an exhalation-valve.
The existence of the mechanism which recognizes that this intake ends is the point which is the most different from the conventional ventilation mode.
3. The control
system
1) The controlling mechanism
Two methods are used for the intake controlling mechanism of PSV.
a) The electronically controlled method
The mechanism which used the graduate-acting control valve (the servo valve) which depends, being electronically controlled is general.
900 C of Servo, Bird 8400, Benette It is used in 7200, Bear-5, the equal resemblance.
b) The mechanical method
By the demand of the patient by the (
figure ; demand valve : airway pressure
) that gas is output (until the demand of the patient is satisfied) until the airway pressure of the piston is pushed to the Kyoto and its vicinity and opens a ball valve. becomes standard pressure when declining from the PEEP/CPAP pressure
The other one uses demand valve (Demand valve) usually by the mechanism which controls an inspiratory-pressure mechanically (CPU-1żBear-3żCV-4000).
Generally, there are few maximal flows in the mechanical method (However maximum 120LPM).
It is slow in response.
Also, the small index can not be controlled.
2) The operating principle of PSV (The intake control)
a) The intake beginning recognition method
(1)
There is a three direction system of the trigger by the float rigger (2) pressure trigger (3) multi sensor.
For the details, it refers to the clause which is (a
1-c trigger mechanism).
PSV begins only when the intake of the patient is recognized.
b) The start-up control of intake
At the large majority equipment, with the start-up speed of intake depending on the ability of hard, generally, start-up is done with the maximum supply possible intake gas flow rate.
At the low equipment, it takes time by standing up to the PSV pressure and this becomes the pattern of the Pressure cycle ventilation and the similarity.
On the other hand, because pressure is rapidly gained by the respiratory tract when the PSV pressure exceeds 10 cm at the equipment that the maximum supply possible intake gas flow rate is high, it brings about strong pressure psychologically.
There is equipment which is adjusting start-up speed actively, too, in.
Currently, it understands 2 methods of the ironhand type and the control of flow type.
However, as for the start-up flow rate in PSV, an enough research isn't done.
(1) The
mechanism
dependence
type
The one where the start-up speed depends on the performance of intake gas generator Ź\
It starts by the maximal flow for which it is possible to shrink.
(Ex. ; ART-2000, CV-4000, BEAR-5, Bird The 8400th prize)
(2) The
ironhand
type
As for Evita, the start-up speed with PSV pressure is variable with the pressure index type.
In other words, the goal pressure rises with the passage of time but the servo control which made this pressure a standard operates.
(3) The
control of
flow type
Adult-Star is a flow rate index type and in the start-up aspect, there is it in the servo control to become a constant gas flow rate.
According to the setting of PSV pressure, the intake gas flow rate changes.
The higher it sets PSV pressure, the earlier the start-up flow rate, too, becomes.
ü@
c) The control during intake
After the set-pressure (the PSV pressure) achievement, a servo valve (the demand valve) is adjusted to
maintain this. (= The servo control by the pressure)
The poor total pressure (=100cm H to be of the exhalation-valve2It is closed at O degree ).
d) The way of recognizing that
intake ends
The condition to end the inspiratory-phase of PSV is called an end-of-suction end recognition condition but has a various method.
(1) The relative value with
intake flow rate (The
decreasing-rate)
This method is most often used.
If falling to 20-30% of the maximum current velocity (PSV peak flow rate) that intake current velocity was measured, it ends end flow rate (terminal flow rate) and assuming intake.
This method is Bear-3, Bear-5, Bird It is used for 6400, 8400, Servo-300, the 900th prize.
Incidentally, in Bear-5, the % value changes with the setting of PSV pressure.
In Servo-300, 5% of values are used but in Servo-900, 75% of values are used.
(2) The absolute value
of the intake flow rate
decline
It ends intake if becoming below the absolute value with constant intake current velocity.
This is Benette 7200ae and Engstrom Elvira, Erica, Ohmeda CPU-1, IMI CV-4000, Adult-Star adopt.
Intake ends when declining to "the intake trigger level" in Engstrom in 4LPM in Adult-Star when declining in 20LPM in CV-4000 when declining in 10LPM in Benette.
(3) The
others
The end flow rate of New-Port E-200 is the value of about the 0.5th power with maximum current velocity.
The basis which this value was used for isn't published.
The method of the Drager Inc. is unique and is changing a condition, dividing PSV in the start-up period and the pressure maintenance period.
In the time when the intake current velocity stopped in the start-up period, in the pressure maintenance period, it ends intake at 25% of values to the highest value for expiratory flow.
e) The end-of-suction end recognition
condition (The use condition)
In addition to the detection of the intake flow rate decline, a condition below is often used.
(1) The limitation on
the maximum intake
time
E-200 and Benette It is limited to a maximum of 3 seconds in 7200ae, Hamilton Amadeus, Veola, in Adult-Star, it is limited to 3.5 seconds, in CPU-1, it is limited to 1 second, in Evita, it is limited to 4 seconds and it is limited to 80% of the IPPV cycle time in Servo-300 and Servo-900.
(2) The limitation
on the airway
pressure
Moreover, there is a model to have added the rise of the airway pressure to as one of the
end-of-suction end conditions. PSV pressure + 3cmH to be by Adult-Star and Servo-9002In the O, it is Benette PSV pressure + 1.5cmH to be by 7200ae.2PSV pressure + 2cmH to be by E-200 in the O2Servo-300 preset Pressure Control Level above PEEP + 20cmH to be in the O2PSV aborts in the O.
(3) The
limitation on
the intake
quantity
An inspiratory-capacity is limited in New Port E-200 and VIP Bird. The former is 4ćg, the latter is
1.5ćg and PSV aborts.
4. The modification
element
1) The maximum current velocity which it is possible to supply
In PSV, the maximal flow which it is possible to supply, too, is an important element.
Of the patient that the ventilating mechanism declined remarkably however, about 80 l/min of the maximum intake current velocity are observed and the able-bodied person reaches 200 l/min, too.
Therefore, the thing with big supply maximum current velocity is the causa sine qua non of the PSV success.
At the latest resuscitator, equal to or more than 120 l/min are possible and are VEOLA, AMADEUS, Benette At 7200, it is 180 l/min.
However, because the domestic machine of the part can supply only about 60-70 l/min, the method which makes up the lack of distributed-gas, floating down a continuous flow is taken.
However, because the continuous flow can point to the time which does a trigger by the protraction, compromise the original advantage of PSV by this.
Moreover, the flow rate in the early stages of intake is remarkable and PSV is high and also because the rates which the intake quantity this time accounts for in the total-ventilation are many, to get the same air quantity of ventilation, the higher PSV pressure becomes necessary.
The higher the PSV pressure is, it becomes difficult to reflect the will of the patient in the ending of intake more and a the more compulsory character like the pressure cycle ventilation it strengthens.
Originally, the continuous flow and PSV should not use the heterogeneous ventilation law chopper eyes which pull a leg each other (The float rigger is different).
2) The driver reaction time
The delay which does a trigger from the beginning of the spontaneous-respiration has changed the character of PSV because it requires the higher PSV pressure by the reason which is the same as (1).
5. The advantage and the fault of
PSV
There is an advantage for which it is easy to reflect the will of the patient in the Å]ł│ type artificial breathing like PSV but to fall into "the lack of the air quantity of ventilation" is given when the spontaneous-respiration becomes feeble as the fault and an airway resistance is increased.
Also, it has been left just as it is if the spontaneous-respiration passes away as the fault which is peculiar to PSV.
Therefore, the expired volume per minute monitor, the (b) anaerosis back-up (Apnea Back-up) feature of the (a) expiration are indispensable for PSV to prevent malpractice.
Moreover, the back-up mechanism to compensate for the (c) air quantity of ventilation is used by the recent resuscitator.
6. Various air quantity of ventilation
compensating machine Ź\
1) Air quantity of ventilation compensating machine Ź\ to use in PSV
a) The PSV + anaerosis back-up (Apnea back-up)
When the spontaneous-respiration stops, it is the mechanism which gives active-ventilation (Volume ventilation).
It doesn't compensate for the enough air quantity of ventilation but as the measure when the spontaneous-respiration stops at least, it is valid.
But, if the spontaneous-respiration is in the incompleteness, there is a fault which has been left even if the expired volume per minute declines.
b)PSV+SIMV
It is the realistic way of compensating for the air quantity of ventilation most surely.
The patient can not adjust the rhythm of the spontaneous-respiration to the rhythm of the active-ventilation because the intake work volume should decrease, but it makes actually and doesn't have regularity theoretically in the sunset of the active-ventilation when the fault of this law increases the number of times of SIMV.
Therefore, there is a limit in the reduction of breathing work volume.
At the same time, the patient feels dyspnoea and becomes a psychological stress, too.
Siemens Servo There was a fault with the SIMV number of times which changes according to the breathing rate of the patient, but the estimate of the following active-ventilation by the patient about the SIMV method which was used for 900B was possible and could adjust rhythm to it.
This method isn't regrettably used for a recent resuscitator.
c)PSV+EMMV
It supports a spontaneous-respiration in PSV and it is the method which makes up the shortage of the air quantity of ventilation with the active-ventilation by EMMV.
However, it does shallow PSV of Ģpē± (if the ventilation capacity is insufficient) when however, the patient will escape from a few active-ventilations because EMMV is the ventilation law where the active-ventilation is standing by as "the punishment".
It isn't desirable even if it sees this condition from the ventilation efficiency and also the stable respiratory condition which is attended by PSV+SIMV, too, isn't gotten.
That general PSV+EMMV doesn't exceed PSV+SIMV and to think that it does the back-up mechanism of the high level to PSV go out of the reality target.
However, as for EMMV (written with MMV in Evita) of the Drager Inc., because appropriate filtering processing is done to the characteristic which is peculiar to EMMV such as the periodic change of compatible and the expired volume per minute to the anaerosis, the usability is high with following above AMV.
d)PSV+AMV(Augumented Mandatory Ventilation)
It is loaded into Bear-5.
It is a ventilation law with the back-up feature by EMMV which PSV+SIMV had.
Because the optimal value with the SIMV number of times is wide, the advantage of this ventilation law lies in the point which flatters flexibly even if the change is in the condition of the patient.
Therefore, there is not necessity which makes a setting change Ģpē±.
e)VAPS(Volume Assisted Pressure Support)
ü@
2) Air quantity of ventilation
compensating machine Ź\ which controls
PSV pressure
a)MMV(Minimum Minute Ventilation)
To distinguish from the abbreviation of Mandatory Minute Ventilation, since then, it is called Hamilton-MMV.
It is the ventilation law which the Hamilton Inc. proposed and it is the ventilation law which adjusts PSV pressure automatically for a stable expired volume per minute to be gotten.
The PSV pressure doesn't become below the set value.
MMV functions with the back-up mechanism and the incorporation which was named Step by Step Procedure and of the low expired volume per minute in addition to the anaerosis however, it switches over to the back-up by SIMV.
b)VS+PRVC
It is the new ventilation mode to have been loaded into Servo-300.
VS(Volume Support) is ĢŽ¢@ of PSV and achieves the stabilization of the air quantity of ventilation in controlling PSV pressure automatically in the concept like Hamilton-MMV.
The minimum PSV pressure can not be set.
PRVC(Pressure Regulated Volume Control) is prepared as the anaerosis back-up of VS.
(For
details, it refers to chapter of II-14.VS+PRVC).
{kind=link}