VIASYS
AVEA
The VIASYS Inc. is the parent company of the Bird Inc. and the Bear Inc..
AVEA which was sold in 2002 is the successor species of the Bird resuscitator series but Bear series successor species however, there is it at the same time.
AVEA is the high performance aeroplane which was developed as the rival of Evita and Servo i.
Of course, it supports a newborn baby-an adult.
On the other hand, AVEA when changing a viewpoint is the host computer of the intake valve method and Vela is the host computer of the turbine method.
Of the equipment which makes a pair each other however, there are these.
The outward appearance and the operation are Vela and similarity and operability by the touchpanel and moreover latest breathing mode to contain NIPPV are made the graphic display feature of 3 corrugations which used an electrochromatic display, being fully equipped, being average.
There are 2 models of Standard (6,200,000 yen) and Comprehensive (9,200,000 yen) in AVEA, too.
The difference is the existence or non-existence of built-in of the (1) stand (2) compressor, the right or wrong of the (3)Heliox supply.
Of course, it is possible to make an option develop into Comprehensive by adding it to the Standard model after purchase, too.
2. The
performance
1) The mode that it is possible to use
A/C
SIMV+PSV
CPAP(PSV)
NIPPV
APRV/Biphasic (Except the newborn baby mode)
---------------------------------
+VCV
+PCV
+PRVC
+ TCPL (Only the newborn baby mode)
+Vsync
+PEEP
+Apnea Backup
2) This proximal dater
The maximum intake gas
flow rate
The active-ventilation .150LPM
PSV.
Above .180LPM
The number of the maximum active-ventilations .120
BPM (The infant and newborn baby 150BPM)
The maximum SIMV number of times .120 BPM (The
infant and newborn baby 150BPM)
3. The explanation of the control
circuit, the controlling
mechanism
1) The outline of the controlling mechanism
If expressing like an image, it is VIP Bird and Bird 8400, Bear 5, Bear 1000 seems to have united in the development and there is 1000.
All breathing modes and a mechanism are had.
2) The characteristic of the mechanical mechanism
The method that the microprocessor controls an intake servo valve and an expiration servo valve is adopted.
It ventilates by the mechanism to relieve the continuous flow the TCPL mode, OBJ DO and which is expressed, adding heat ray type Fluothane Sir to the Y peace to the newborn baby in the pressure by the exhalation-valve.
3) The gas flow rate measurement
It measures a gas flow rate on the side of intake by the delta-pressure type.
A gas flow rate on the side of the expiration is measured with the delta-pressure type flow transducer of the film type.
In the TCPL mode, it installs a heat ray type flow transducer between the tracheal tube and the Y peace and it measures the intake and expiration gas flow rate.
4) The intake valve
The intake valve that the servo control which is the same as Bird and so on 840 was done is used.
5) The expiration valve
It is the film type valve of the servo control type. It is directly
driven with the linear motor.
It is Bird840 and similarity but a new Mattick circuit is more simplified.
There is not an entry in the figure but an entry for Heliox, too, is prepared with the option.
Therefore, the adjustment of the oxygen concentration and so on becomes easy and can use Heliox safely.
Oxygen and compressed air are decompressed respectively by the same pressure with the regulator after passing a filter.
It is adjusted in the boiling that the oxygen-tension, too, is the same as air because the standard pressure becomes air pressure about the regulator (being Relay and an entry in the figure) on the side of oxygen.
Next, it is controlled in the entering, the oxygen concentration by the blender.
A blender is the same as Bear1000 and is controlled with the stepper motor.
It is checking pressure with pressure sensor (Blended Gas Pressure Transducer).
If there is a difference normal pressure, the pressure of system's being extraordinary and becoming is released in the big worrying.
Coal-water-gas becomes intake gas in intake gas with intake valve (Flow Control Valve), being controlled.
Station on the way, pressure and a temperature, a flow rate are measured.
At the equipment abnormality time, Safety Relief Valve which releases intake gas in the big worrying is provided.
After passing a filter, the flow measurement of the delta-pressure type is done and expiration gas is released in the big worrying by the exhalation-valve.
Moreover, as for the exhalation-valve, the drive-system that response was improved is used from Bird8400.
It becomes the structure which drives an exhalation-valve film directly with the electromagnetic coil.
An drive electric current is adjusted by the microprocessor.
5. The control
software
The explanation of the each function
1) The trigger formula
It is a flow trigger formula. It is possible to set in
the range of 0.1-20LPM.
2)A/C
Ventilation form of quantity ventilation (VC), pressure ventilation (PC), PRVC, TCPL can be chosen.
3)SIMV
In the spontaneous-respiration aspect, PSV can be added. In the active-ventilation aspect,
ventilation form of the quantity ventilation, the pressure ventilation, PRVC, TCPL can be
chosen.
4)APRV/Biphasic
It is BIPAP of the wide sense in the place to say in the Drager Inc..
It changes two pieces of CPAP pressure alternately.
This synchronizes with the spontaneous-respiration of the patient.
In the trigger window time in case of change, it is possible to set in 0-50% of ranges of the time of high-pressure aspect (Time High), low pressure aspect (Time Low).
Moreover, PSV with optional pressure can be added to both of the high-pressure aspect, the low pressure aspect.
Only the low pressure aspect can do boiling, too, in the addition of PSV.
It becomes APRV when setting the time of the low pressure aspect shortly.
The anaerosis back-up, too, can be used.
The anaerosis alarm shifts to the sounding back-up ventilation when not detecting a change and a spontaneous-respiration with pressure above the set-up time.
It returns to the original APRV/Biphasic mode when detecting a change or a spontaneous-respiration with pressure.
5) The quantity ventilation (Volume Ventilation)
There was an intake demand (the demand) by the patient who exceeds a setting intake gas flow rate in case of quantity ventilation.
In the case, because the patient could not breathe in intake gas with part of exceeding a setting intake gas flow rate, the patient felt choking and if anything had the side where the quantity ventilation obstructs the intake effort of the patient.
Already, as for the resuscitator of the Bear Inc., the mechanism which increases intake gas according to the demand to solve this problem was laid down.
This concept is taken over by AVEA, too.
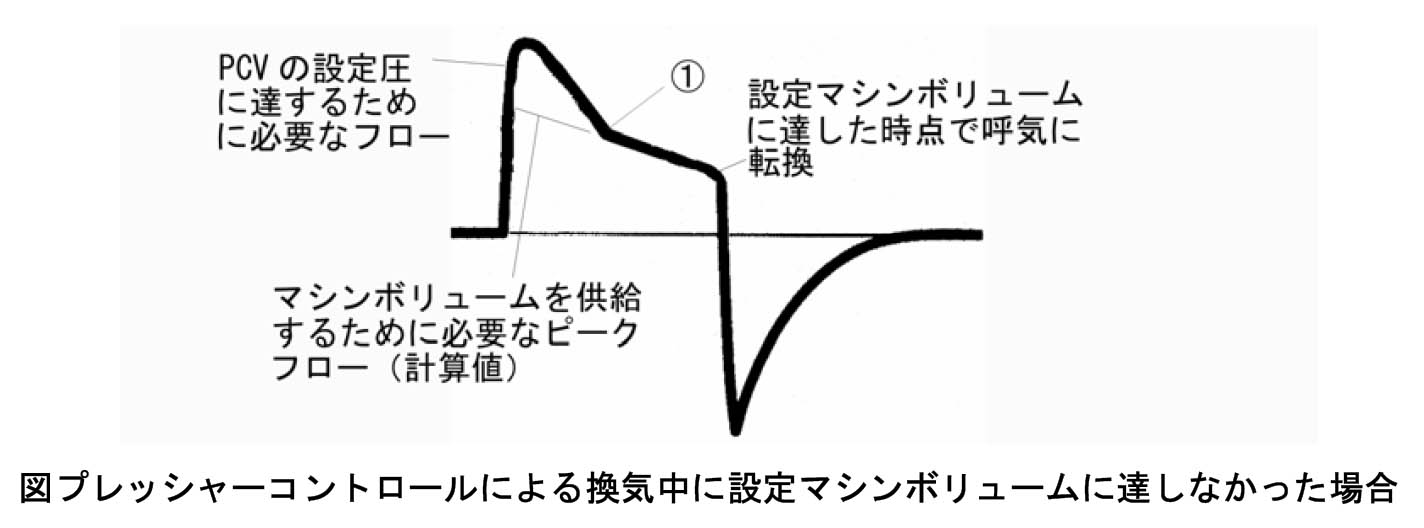
The quantity ventilation in AVEA is the development type of Pressure Augumentation of Bear1000.
Pressure Augumentation is VAPS and the similarity of Bird8400 but as for this concept, a folklore is done to the concept of quantity ventilation demand feature and its following Machine Volume.
Pressure Augumentation is quantity ventilation and the ventilation that virtual PSV starts at the same time if expressing simply.
The quantity ventilation and virtual PSV differ in the intake flow rate pattern (the flow pattern) but the ventilatory-pattern with more intake gas flow rate values when there is moment of intake becomes predominant.
In Bear1000, the demand feature which was named Flow & Volume Augumentation because it supported an intake demand (the demand) by the patient who exceeds a setting intake flow rate was laid down.
As for this, the target pressure of virtual PSV was the demand feature which is done at the PEEP pressure in Pressure Augumentation.
In AVEA, virtual PSV which targetted a measurement airway pressure in some moment of intake-the pressure of 2cmH2O is Pressure Augumentation with the form which is progressing at the same time and supports a demand.
In other words, the target pressure with virtual PSV pressure is the translation which is changing based on the actual measurement.
Incidentally, a minimum is provided for PEEP+2cmH2O by the ventilating-pressure of virtual PSV.
The processing after a setting taking air quantity of ventilation is 送気ed has the following 2 patterns.
(1)
When there are more intake gas flow rates (the intake flow) than the setting intake flow rates, virtual PSV continues continuously.
When the intake flow rate declines to equal to or less than 25% of the highest value for expiratory flow, virtual PSV ends.
(2)
Already, in the taking air quantity of ventilation, because it is necessary to have been 送気ed, the inspiratory-phase ends just as it is in the case that the intake gas flow rate is the same as the setting intake flow rate, i.e. the condition that the demand isn't operating.
6)PRVC
PRVC is the ventilation form which does PCV pressure in the self-regulation to become a setting taking air quantity of ventilation.
A pressure change every ventilation is limited below 3㎝H2O.
The test quantity ventilation (the dwindling wave) which contained the intake pose of 40 mS is done when PRVC begins.
Because a dynamic lung-compliance is measured at this time, the pressure which is necessary to ventilate in the next time can be fixed.
Since the 2nd, it is ventilated by the pressure ventilation and the following ventilating-pressure is fixed from the value of the measurement air quantity of ventilation of the case.
Volume Limit can be set, too.
In Flow Cycle setting, the end-of-suction end by Flow Cycle becomes valid only when the taking air quantity of ventilation can be achieved.
The ventilating-pressure decision process by the test ventilation re-begins at the time of the following condition.
(1)
By the (4) measurement taking air quantity of ventilation that (3)Volume Limit which changed the (2) setting taking air quantity of ventilation to have changed to the PRVC mode was operated
The (6) standby end which the (5) test ventilation stopped on the way when 1. of the set value became quintuple
(7) As for some of the following alarms, when occurring, the high-pressure alarm, the low pressure alarm, the PEEP minimum alarm, the patient circuit are a difference alarm, an intake time limit alarm, I:E limit alarm.
7)PSV
As for the minimum value with PSV pressure, in setting for the adult and the infant, PEEP pressure + 2cmH2O becomes and in setting for the newborn baby, the PEEP pressure becomes a minimum.
8) The anaerosis back-up
The anaerosis back-up is valid in all modes.
It does an automatic-reset to the original mode when detecting a spontaneous-respiration.
It is ventilated by either of the anaerosis time or the setting air changes per hour more air changeses per hour in A/C and the SIMV mode.
There are few cases which operate in the actual validity in A/C and the SIMV mode.
In the APRV/BiPhasic mode, it sets a ventilation condition beforehand by the advance setting in CPAP/PSV.
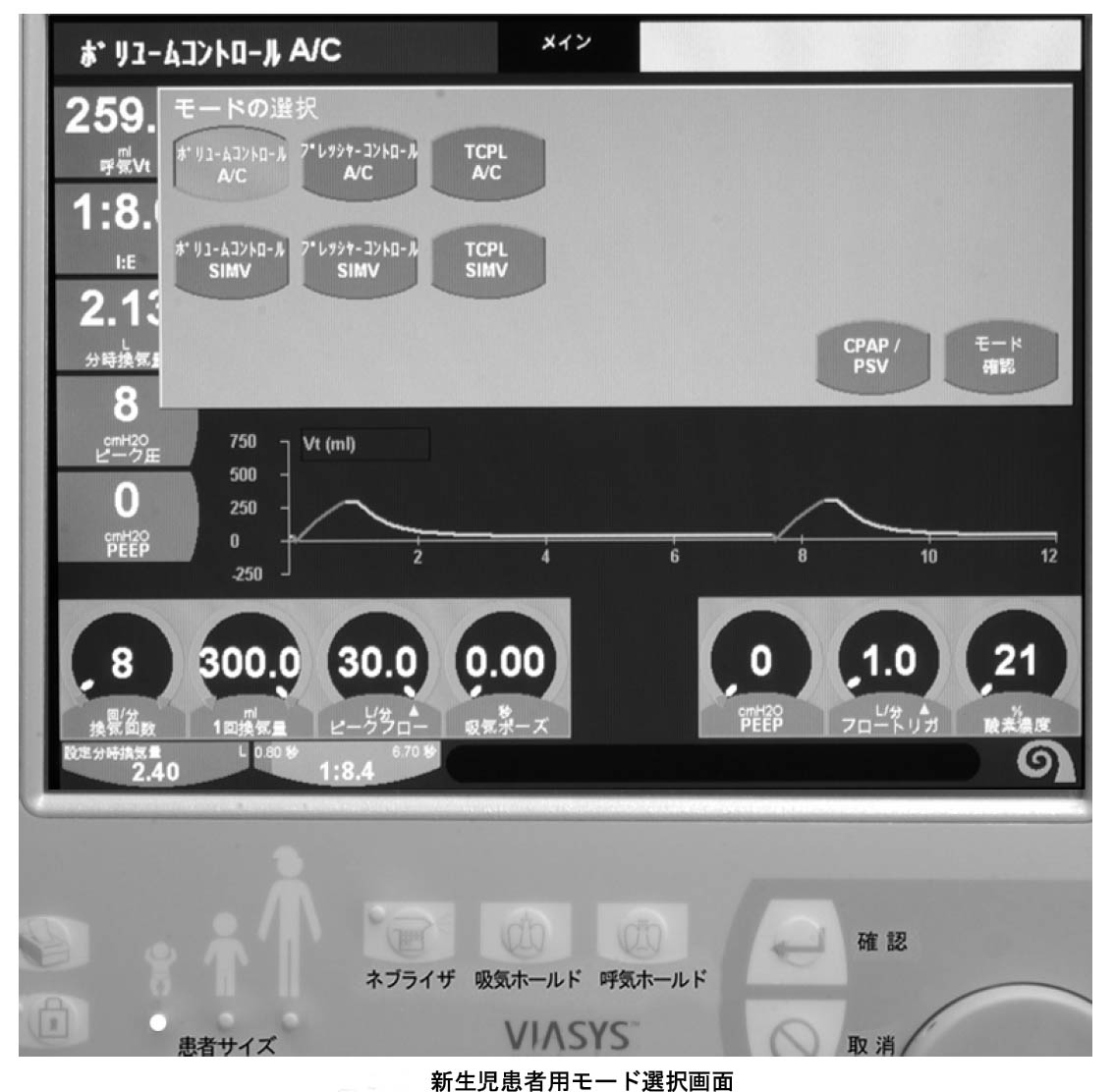
9)TCPL
TCPL is the name of the VIASYS Inc. to the mode (the patient is freely the 換気 mechanism which is used by the resuscitator for the newborn baby because it is possible to breathe anytime in the continuous flow) to make an inspiratory-pressure occur by relieving a continuous flow in the pressure by the exhalation-valve by the abbreviation of Time Cycle Pressure Limit.
It is possible to choose only when setting for the newborn baby.
Because a continuous flow is all the time supplied, because the patient puts on freely with intake even if there is not a trigger, there are few breathing work volumes compared with the demand method.
It is possible to make on only by the pressure ventilation.
In the TCPL mode, it is impossible to operate.
It secures the air quantity of ventilation (off, 0.05-2.0 the large, default value off) which was set by Pressure Augumentation and the VAPS similarity mode.
As the image, the pressure ventilation and the quantity ventilation begin at the same time.
Because the one where there are these more intake gas flow rates is output, it becomes the gas flow rate of the quantity ventilation when the intake gas flow rate decreases by the pressure ventilation in the early stages of intake.
When an air quantity of ventilation is achieved, the inspiratory-phase ends.
11)Flow Cycle
The intake of the pressure ventilation ends when the intake gas flow rate falls to the % value (it is possible to set at 0-30%) to the peak value of the intake gas flow rate in case of pressure ventilation.
In other words, it is possible to make the ventilation of PSV and the similarity when making this on.
12)Volume Limit
It is valid only in PRVC, and Vsync, TCPL, PCV. The intake ends when the taking air quantity of
ventilation reaches a set value (0.05-2.5 the large, default value 2.5L).
13)Vsync
It is valid only in the quantity ventilation.
It becomes the ventilation mode which is the same as PRVC when making on by the quantity ventilation.
As for the point of difference with PRVC, the setting method of the ventilatory-pattern is different actually only.
PRVC is an independent ventilation mode and sets from the taking air quantity of ventilation, the intake time.
On the other hand, Vsync is an added function to the quantity ventilation.
In the quantity ventilation, it sets a taking air quantity of ventilation and an intake gas flow rate and intake time is more automatically fixed than these values.
The in this way set quantity ventilation shifts to the PRVC ventilation when making Vsync on.
14)Wave Form
It is valid only with the quantity ventilation.
The standard is the dwindling wave to fall to 50% of intake gas flow rates to the beginning end in the set value of the intake gas flow rate (the intake flow).
The Comprehensive model can choose a square wave.
But, there seems not to be a merit which can choose a square wave.
15)Sigh
It is valid only in the quantity ventilation. When making on, as for either in ventilation with 100 times or
7 minutes, in the shorter interval, the quintuple taking air quantity of ventilation of 1. is given.
16) The nebulizer
Nebulizer gas comes out with the oxygen of 6LPM only among the inspiratory-phases when making a nebulizer on.
Therefore, the taking air quantity of ventilation increases that the nebulizer is occupied by 100 ml to the intake time of 1 second.
Also, only the part increases in the oxygen concentration, too.
The nebulizer can be set by the unit in 5 minutes until a maximum of 60 minutes.
17) The battery
In case of the power failure, with built-in battery, it is possible to operate for approximately 6 hours.
18) The dater output
The nurse call, the optical fiber output, printer (HP940C), Video Output (256 color, 800x600, the SVGA monitor) can be output.
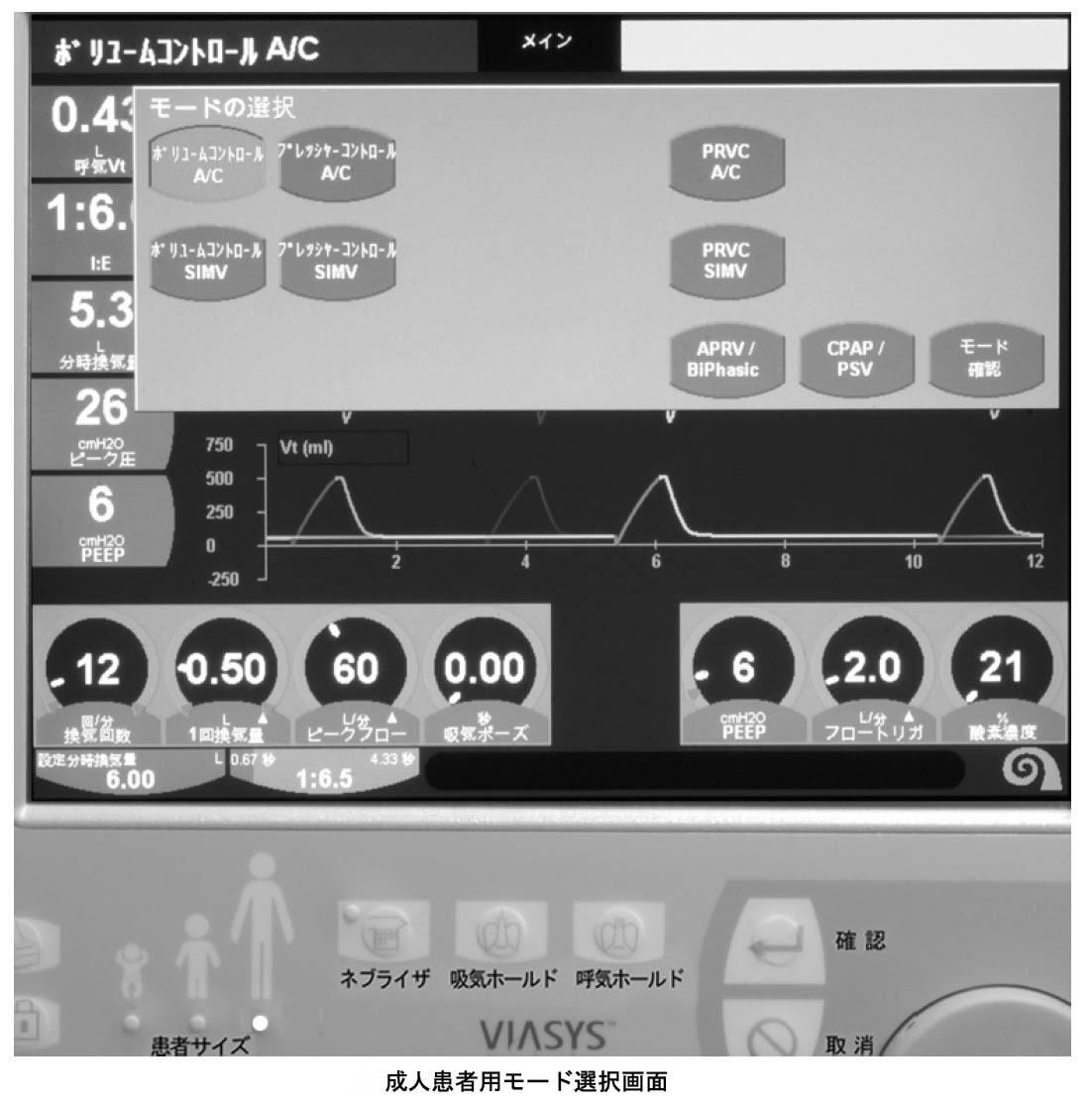
It sets using the button and the touchpanel display in the operating panel right.
It chooses an item in the touchpanel, and a value entry turns and enters a dial and is fixed in ACCEPT (the understanding).
2) The environment operating
It becomes the screen which chooses first RESUME (resuming by the setting in the last time) or NEW PATIENT (new 患).
It becomes the screen which chooses a humidifier next when choosing and ACCEPTing (the understanding) either.
It chooses HME or a heating humidifier.
Next, it chooses a mode.
Because the item which it should set according to the mode is displayed, it inputs value to them.
The setup button for the anaerosis back-up appears only when choosing APRV/BiPasic, CPAP/PSV, NIPPV/CPAP PSV.
It enters the value which needs this, too.
3)ADVANCED SETTING
If the more advanced setting is necessary, it presses the ADV SETTING button which is in the lower right of the touchpanel.
Machine Volume, Flow Cycle, Volume Limit, Vsync, Wave Form, Sigh, Bias Flow, PSV Cycle, PSV Tmax, Time High, Time Low, "NADOWO" can be set.
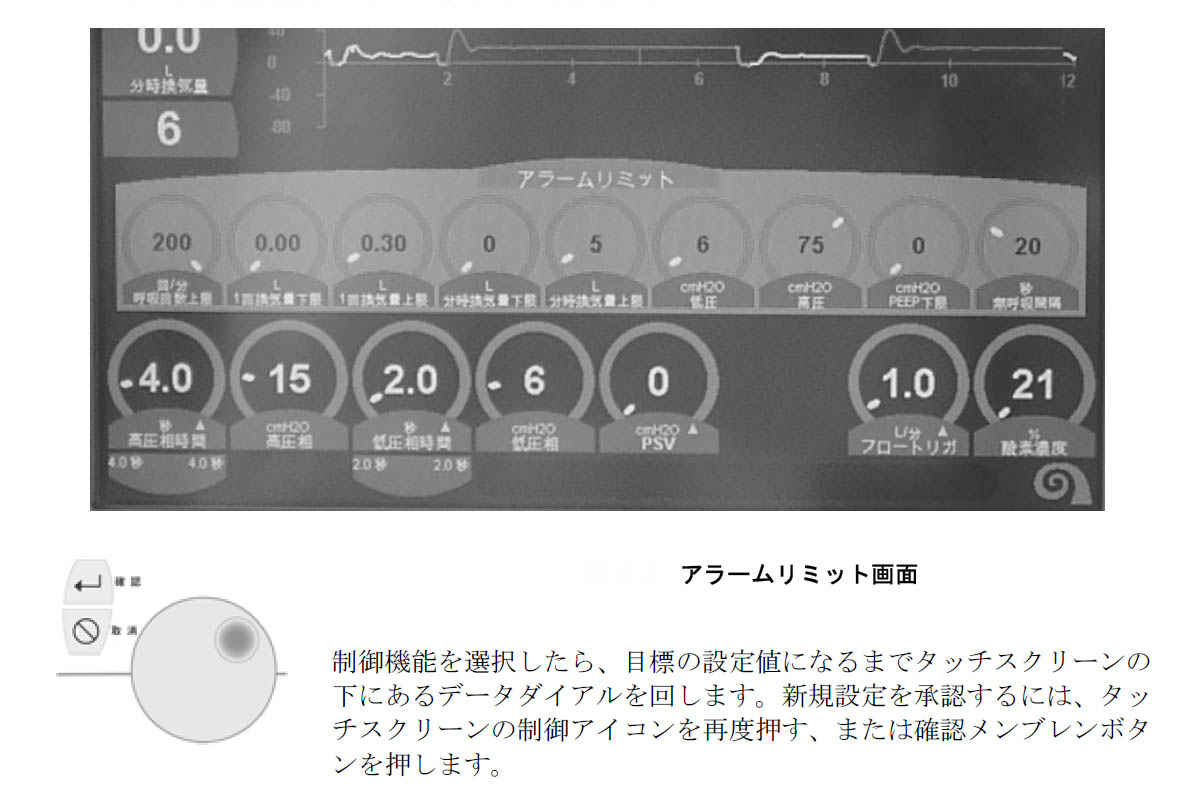
The low expired volume per minute, the air changes per hour excess, the low taking air quantity of ventilation, Low PIP (the airway pressure minimum), High PIP (the airway pressure upper limit), Apnea (the anaerosis time), the "NADONO" item can be set.
It sets using the touchpanel and the dial.
It is possible to display in the large-sized electrochromatic display touchpanel.
Because a screen selection menu is displayed when touching the place to be displayed, saying "mainly" at the center of the finial in the touchpanel, it changes a screen-display using this.
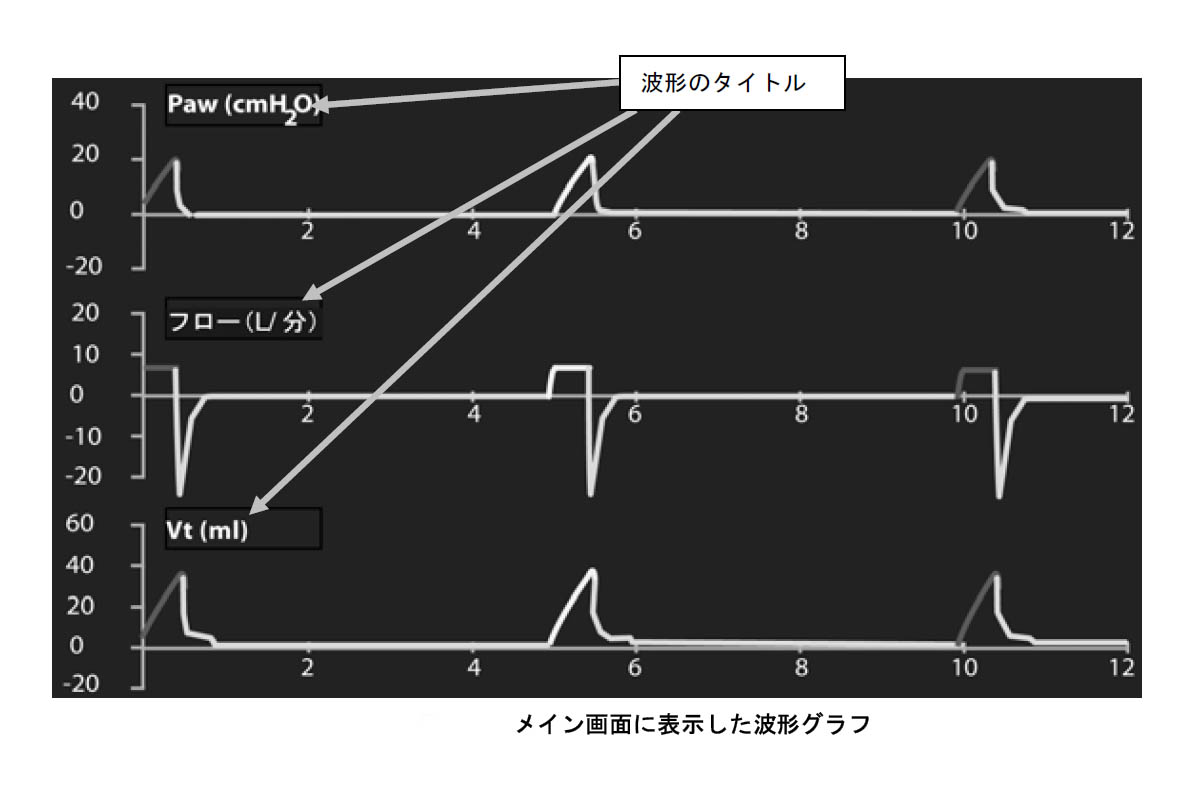
The air quantity of ventilation, gas flow rate, airway pressure graphic of 3 corrugations can be monitored.
The inspiratory-phase is red and an expiratory-phase is displayed in the blue.
The scale can be chosen in the touchpanel.
The Comprehensive model can measure LOOP, TRENDS, Maximum Inspiratory Pressure, Negative Inspiratory Force, AutoPEEP, a static-compliance and so on.
As for the humidifier, the F&P type is come equipped with.
10. The daily maintenance
1) The daily life
It washes regularly in the resolution according to the protocol which could specify breathing circuit, an exhalation-valve, expiration Fluothane Sir and so on at the patient hospital and it is sterilized.
11. The regular
inspection
It receives regular inspection by IMI in 6 months, 1 every year. It exchanges if checking the
capacity of the battery, too, regularly and being necessary.
12. The fault
1) It evaluates a multifunction point but it is necessary to organize an interface and a concept.
In the possible mode, even if it is completely displayed at the operating panel, the operation and the concept are too complicated.
It is anxious for the mis-setting by the mistake.
It becomes the more simple operation system if the user can choose a display item and makes only a necessary mode and a feature be displayed on the operating panel.
2) The design of the outward appearance isn't good.
Of the exterior, too, twopenny
It hears that it unified the operability of VELA and AVEA but that the outward appearance is similarity for both to have considerable price difference is doing loss like an image.
3) When maximum of incorporating the request of RT, such a resuscitator will be made but that there is not a clear policy on the side of the development is irresponsible in a sense.
It should distinguish between "the indispensable feature" of the resuscitator and "the feature which is convenient if being", being clear.
For example, the feature not to use of? too much should make access with the back screen and so on about whether it isn't enough only in any one such as Vsync and Machine Volume, PRVC.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}