Puritan Bennett
840
The Puritan Bennett Inc. is rather the few long-established store which continues to produce a resuscitator than the incunabula (1940 marriageabilities) of the resuscitator.
It was involved in the storm of station on the way, M&A (the corporate acquisition), and in 1995, it was bought by the Nellcor Inc. and it became Nellcor Puritan Bennett.
In 1997, Nellcor Inc. was more bought by the Mallinckrodt Inc. and Puritan Bennett became 1 brand of the Mallinckrodt Inc..
After that, it was bought by the Mallinckrodt Inc. "TO" Tyco Healthcare group and Puritan Bennett became the part gate of the Tyco Healthcare group.
Puritan Bennett is Bennett of the sale in 1984 It is the sharp "NO" brand which brought the progressive mechanism which becomes the foundation of the resuscitator today with 7200 to the industry but it hears that it was behind in 840 pieces of development in with the confusion of M&A.
It is becoming Bennett gradually in 1998 840 was sold.
It is possible to support from newborn baby (3.5Kg) to the adult and it is Servo It grew at 300 powerful rival products.
Specifically, as for the pressure ventilation mode, improvement is added and like the BIPAP system of the Drager Inc., because the exhalation-valve, too, participates in the inspiratory-pressure control actively, there are few overshoots and they make stable pressure maintenance possible.
The Flow Acceleration % of PCV, PSV and the Expiratory Sensitivity % (the end-of-suction end recognition flow rate) of PSV, too, can set a user.
Ex-model Bennett The display ability which was 7200 defects and the operability became the display for DualView Touch Screens Display to understand and the operation it is easy understand.
An exhalation-valve controllability, too, was substantially improved by the active control.
A compressor, a back-up power are prepared as the hardware option.
The software option mode includes Volume Ventilation Plus, Bi-Level and PAV, NeoMode, NPPV.
An object is expanded into the newborn baby with 0.5-Kg weight if equipped with NeoMode.
2. The
performance
1) The mode that it is possible to use
A/C (PCV,VCV,VC Plus)
SIMV(PCV,VCV,VC Plus) + PSV
SPONT(CPAP,PSV,VS,PAV,Bi-Level,NIV)
---------------------------------
+PEEP
Flow trigger(Flow-by)
Apnea Backup
NeoMode
Bi-Level
ü@
2) This proximal dater
The maximum intake gas flow rate
The active-ventilation
.150LPM
PSV. .200LPM
The number of the maximum
active-ventilations 100
BPM
The maximum SIMV number of
times .100 BPM
The battery drive time Built-in battery ; Equal
to or more than 0.5 hours
ü@
3. The control circuit, the
controlling mechanism
1) The outline of the controlling mechanism
It is using Motorola 68040, 24Mhz for MPU.
It is used for breath delivery unit (BDU) and graphic user interface (GUI).
Two MPU are watching over the operation status mutually.
2) The characteristic of the mechanical mechanism
The patient circuit is two simple tubes of the Bennett style and an exhalation-valve and Fluothane Sir are protected by the large-sized filter.
3) The gas flow rate measurement
An expiration gas flow rate, an intake gas flow rate are measured with the hot film type sensor.
4) The intake valve
It is equipped respectively with the flow-control valve which is called PSOL to oxygen and the air. It does
the control of the oxygen concentration and the control of the intake gas flow rate like a lifetime.
5) The expiration valve
At 7200, it was a mechanical control but at 840, it was improved in the servo control method.
It maintains PEEP pressure actively so as not to be influenced by the change of the flow rate of expiration gas.
This is called active exhalation-valve.
Inspiratory-phase however (like BIPAP of Evita), in pressure ventilation, it operates to miss the overshoot of the inspiratory-pressure.
Oxygen, the dense fog which was entered than the air plumbing are decompressed respectively with filter (F1,F3)(F2,F5), non-return valve (CV2)(CV4), regulator (REG1)(REG2).
Mix proportion percentage and a flow rate are adjusted to these gases with flow-control valve (PSOL1)(PSOL2).
The gas flow rate which passes PSOL1, PSOL2 is measured by Fluothane Sir (Q1)(Q2) and is used for the control of PSOL1, PSOL2.
When the patient circuit internal pressure rises extraordinarily at the equipment abnormality time, relief valve (SV) releases an open circuit.
As for the sensor of the airway pressure, the side (P2) of intake and the side (P3) of the expiration are provided.
Solenoid-controlled valve (SOL1)(SOL2) is for the zero point proofreading of the pressure sensor.
A throughput is adjusted to expiration gas by active exhalation-valve via pressure sensor (P3), check valve (CV5), Fluothane Sir (Q3) after passing a heating filter.
5. The control
software
1) The trigger formula
The pressure trigger formula, the flow trigger formula can be chosen.
Piesthesia degree 1ćpH2O, flow sensitivity 1 LPM (the infant), 1.5 So as not to generate an auto cycle when setting more sensitively than LPM (the adult), filtering algorithm is incorporated.
a) The flow trigger
It is trigger sensitivity + 1.5 when choosing a float rigger The base flow of LPM is automatically added.
Also, the pressure trigger of - 2ćpH2O is used as the back-up.
The flow sensitivity is 0.5-20 It is possible to set in the range of LPM.
The original value is 3 LPM(>24Kg IBW) , 2 LPM(<24Kg IBW) Being.
It doesn't become Flow by because there is not necessity in the float rigger.
When operating NeoFlow option (IBW<7Kg), the trigger sensitivity can be chosen in the range of 0.1-10LPM.
There is not a function to revise trigger sensitivity to the leak by the cuff pear tube.
b) The pressure trigger
In pressure trigger choice, it is 1 The base flow (the way of calling changes with the bias flow at the pressure trigger) of LPM is added.
The piesthesia degree can be set in the range of - 0.1-20ćpH2O.
The original value is - 2ćpH2O.
At the pressure trigger, Flow-by operates.
2)A/C
Help or an active-ventilation mode is called A/C.
The pressure ventilation or the quantity ventilation can be chosen (Generally, the former is called PCV and latter is called VCV or sCMV).
An overshoot's there being part is released from the exhalation-valve (like BIPAP) because an exhalation-valve is goal pressure and is closed in the pressure ventilation.
In the quantity ventilation, the flow pattern can be chosen from the square wave, the dwindling wave.
In case of the dwindling wave, it declines from the setting flow rate.
Because the average-stream-flow of the dwindling wave is square wave it a half, in the intake time, it becomes by approximately twice.
The intake plateau can be added.
Whatever ventilation it is, it doesn't accept the setting that the I:E ratio becomes equal to or more than 1 4:, setting with the intake time which becomes from 8 seconds to 0.2 seconds, setting with the expiration time which becomes below 0.2 seconds.
3)SIMV
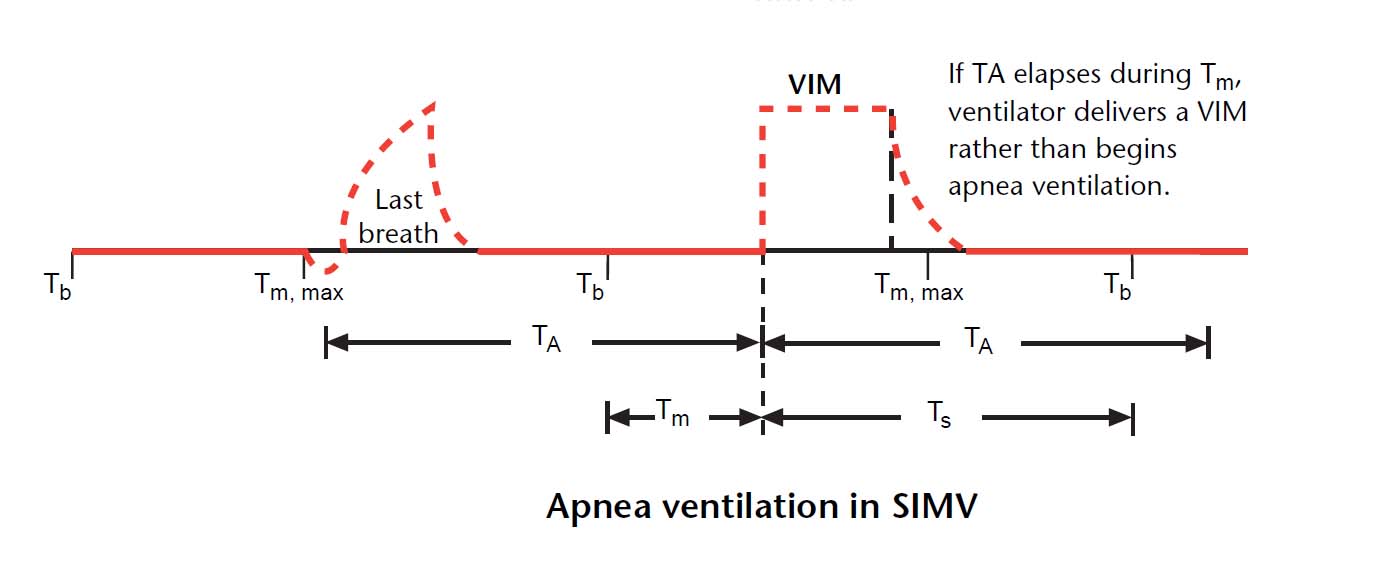
By the fixed time method, it is set to 60% of the SIMV cycle time but the trigger window is until a maximum of 10 seconds.
When the spontaneous-respiration which began with the spontaneous-respiration aspect continues even if the active-ventilation aspect begins, the active-ventilation doesn't begin and in case of extremely, the singular or more than one active-ventilation is omitted.
So as not to enter an anaerosis back-up immediately in SIMV, it puts an active-ventilation once at the 1st anaerosis time and moreover it is the time when the anaerosis time passed the once again and it enters an anaerosis back-up.
This becomes valid when the SIMV cycle time is longer than the anaerosis time.
For example, in the anaerosis time, it often uses 15 seconds but in this case, the setting of the SIMV number of times is 4 It assumes a condition below BPM (
Figure ; Diagram of anaerosis ventilation in SIMV).
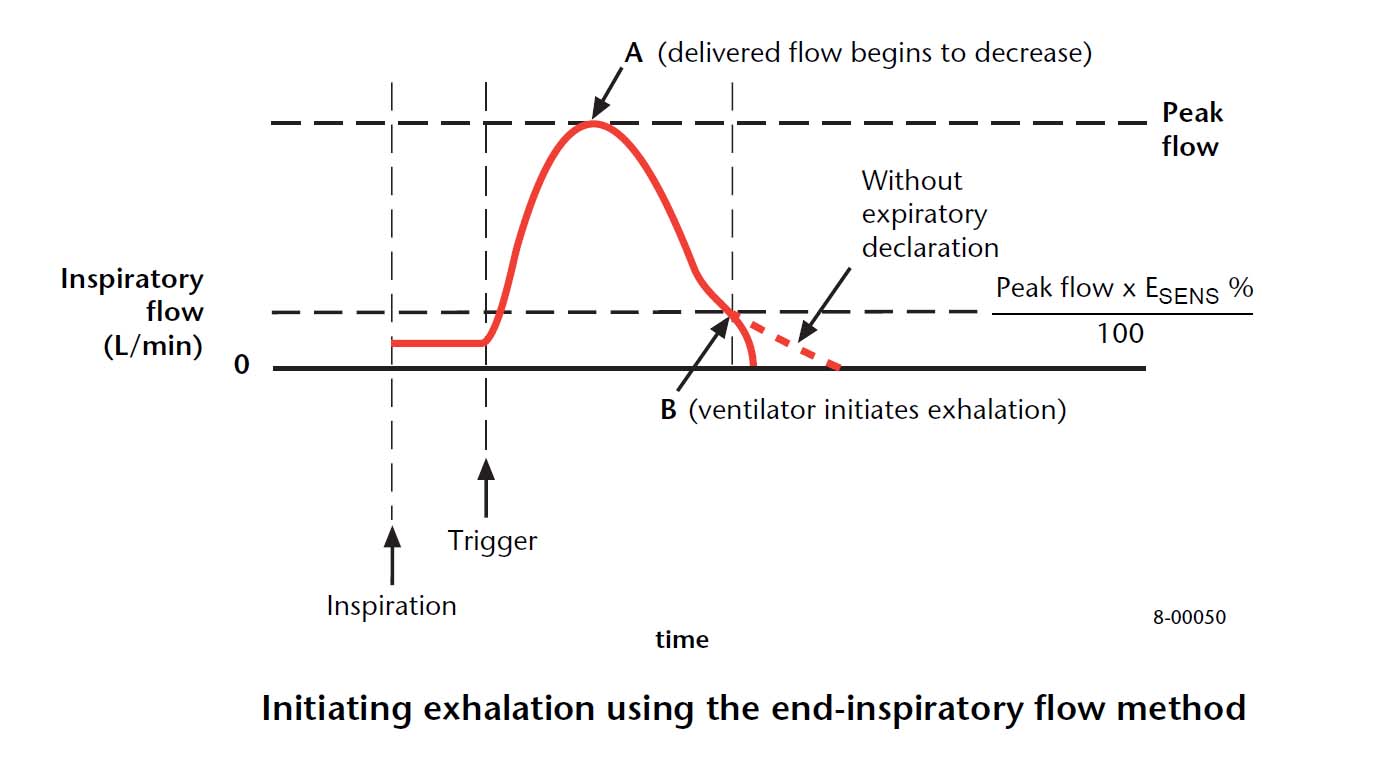
The operator can set inside flow condition (terminal flow) to the end-of-suction end recognition condition.
In other words, the % value to the maximum intake gas flow rate can be set (It is called Esens).
If the intake gas flow rate becomes below Esens, the inspiratory-phase of PSV ends.
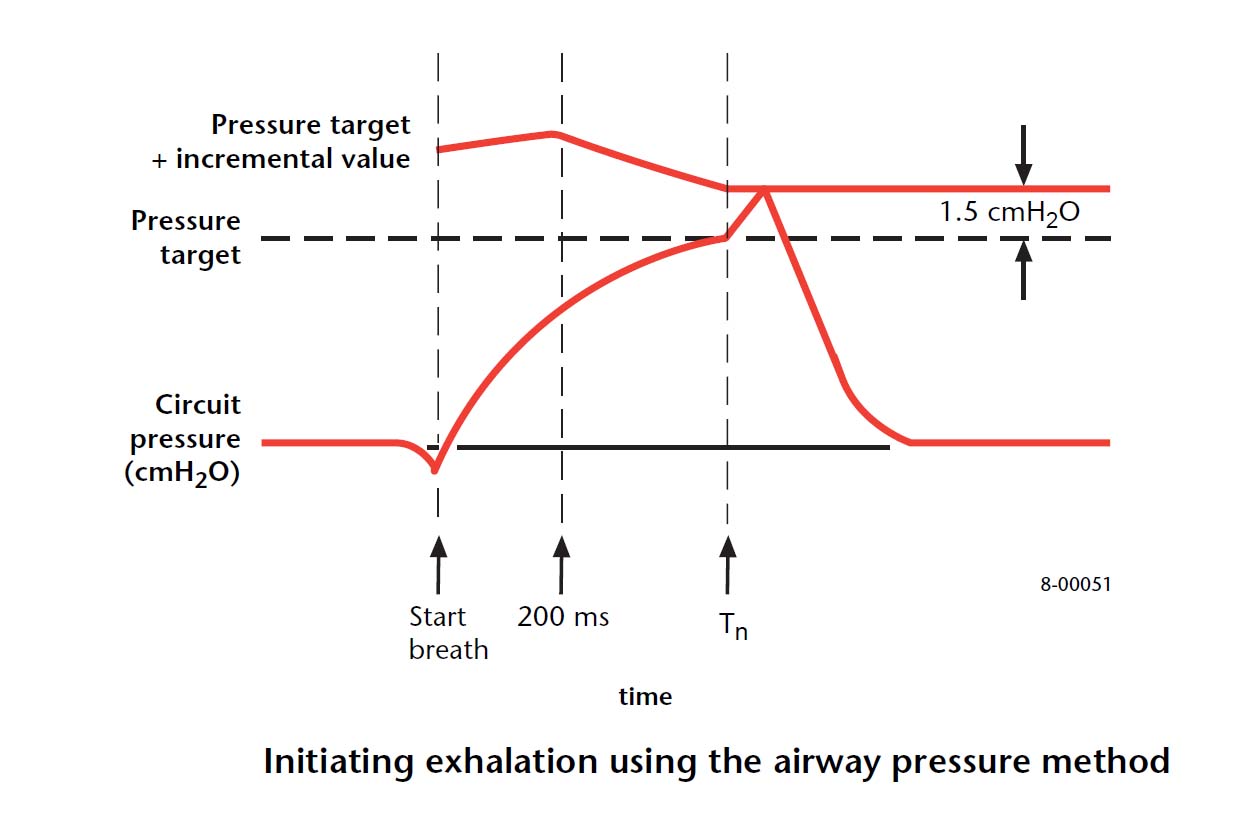
However, when the increment to the goal pressure exceeds a standard value in addition to this, the inspiratory-phase of PSV ends.
The standard value increases straighter to 200 ms than to the intake beginning.
After that, it declines straight in 1.5ćpH2O.
1.5ćpH2O is used since it.
In case of PSV beginning, the one with high standard value is the measure not to cause a malfunction by the overshoot.
A standard value in case of beginning and details with the time (Tn) which declines in 1.5ćpH2O aren't published.
In the maximum intake time, it is 1.99 + 0.02 It is x IBW second.
5) The standing-up flow rate (Flow Accelaration %)
It is possible to set in 0-100% of ranges.
The original value is 50% but the % to something is unclear.
The standing-up becomes early when setting a % value roughly, but it becomes easy to cause an overshoot and an under shot and causes the vibration of the pressure.
Also, because the peak rate of flow, too, increases, in PSV, the end-of-suction end flow condition, too, increases consequently and PSV ends early relatively.
It reaches 95% of the set-pressure in 2/3 in the intake time when setting at least in the boiling.
6)IBW(Ideal Body Weight)
When entering weight when the resuscitator starts, a taking air quantity of ventilation, a maximum-gas-rate, æŚŗC algorithm, an intake time extension alarm as the original value are fixed.
The taking air quantity of ventilation is 7.25 It becomes ml/kg.
The maximum-gas-rate is 80 LPM(IBW<24kg) , 200 LPM(IBW>25kg).
Volume Ventilation Plus(VV+) consists of 2 forms of Volume Control Plus and Volume Support in the general term of the mode which does PCV and PSV pressure in the self-regulation to achieve a setting taking air quantity of ventilation.
The former is used for a controlled-respiration in A/C and SIMV.
In other words, it is the same as PRVC and AutoFlow.
Latter is used by the spontaneous-respiration mode and this, too, is the same as Servo i of the Maquet Inc., and so on.
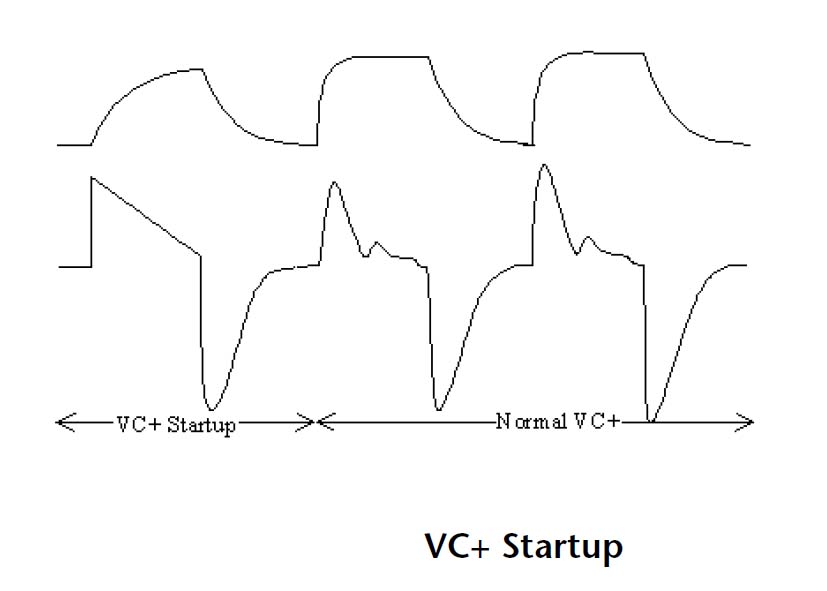
Test ventilation is done at 15ćpH2O or (Peak Pressure)-PEEP-3cmH2O being "DURE" or little pressure when starting up Volume Ventilation Plus.
Since then, it computes a compliance and pressure is done by the self-regulation but a maximum variation is limited like the following table according to IBW.
It explains that it reaches a setting air quantity of ventilation within about 5 breathing.
It is the same as resuming "NOMO" PRVC approximately more than in case of test ventilation when depending on the alarm condition.
ü@ |
The maximum variation in case of pressure control |
ü@ |
IBW>25Kg |
15<IBW<25Kg |
IBW<15Kg |
First within 5
breathing |
+ü[10cmH2 |
+-6cmH2O |
+-3cmH2O |
Since 5
breathing
|
+-3cmH2O
|
The table ; The maximum variation with pressure about VV +
ü@
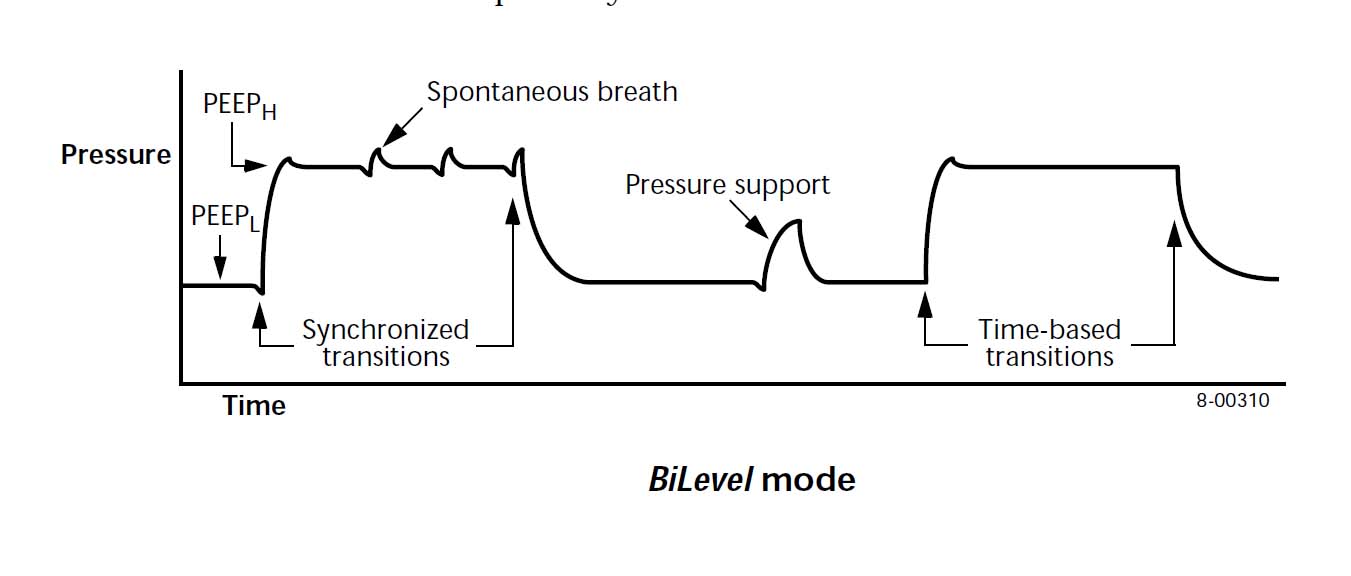
BiLEVEL is BIPAP (of the wide sense) if expressing easily.
PSV can be added to each of the high-pressure aspects and the low pressure aspects.
But, the VYASIS Inc. and so on can choose PSV with optional pressure respectively but in PB840, PSV pressure (the absolute value) with the high-pressure aspect is fixed by the PSV pressure of the low pressure aspect [
Figure ; Explanation of BiLevel with pressure support].
In other words, the separate PSV pressure can not be chosen in the high-pressure aspect and the low pressure aspect.
However, way, because PSV of 1.5cmH2O becomes the theory to be adaptable to about PB840 even if zero piece of PSV pressure meets, in what case, at least, automatically, PSV of 1.5cmH2O is added.
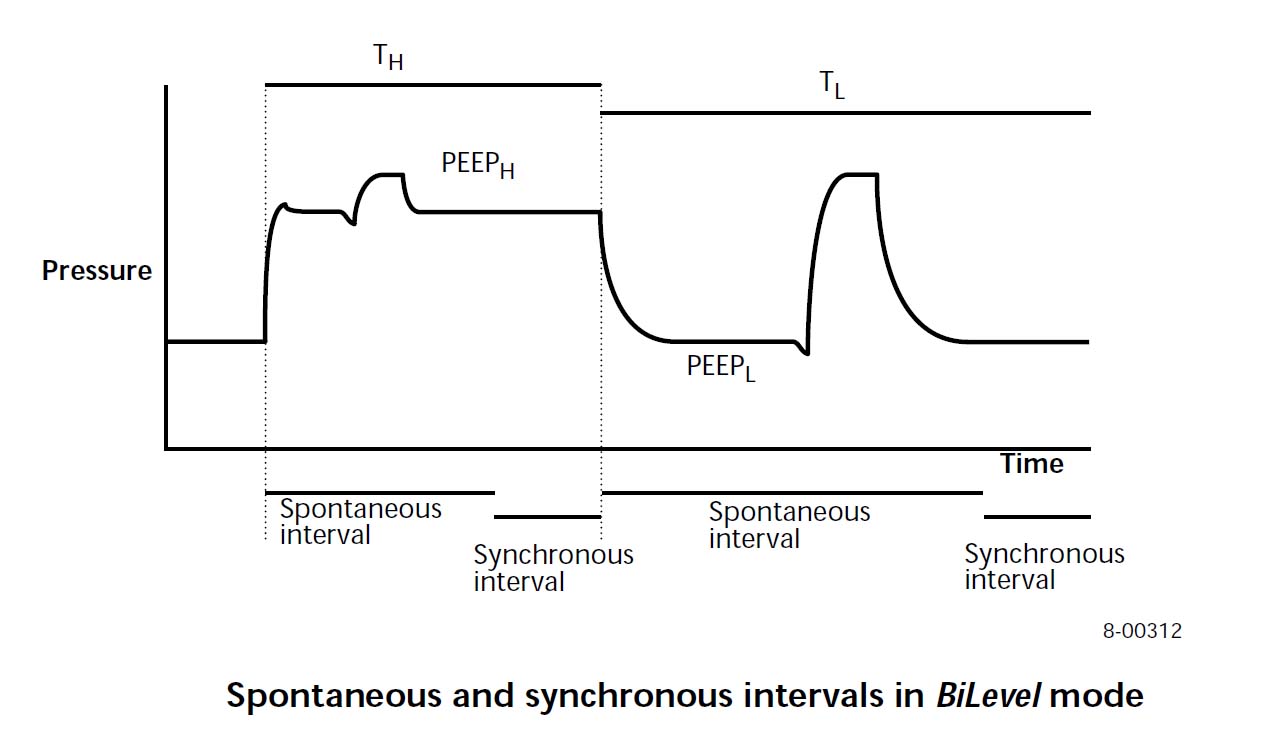
BiLevel can set the time of the high-pressure aspect and the low pressure aspect in the 30-s range.
Therefore, there is a variety which can create APRV and the other pressure ventilation mode.
The trigger window is as in the figure (
Figure ; Diagram of trigger window in BiLevel).
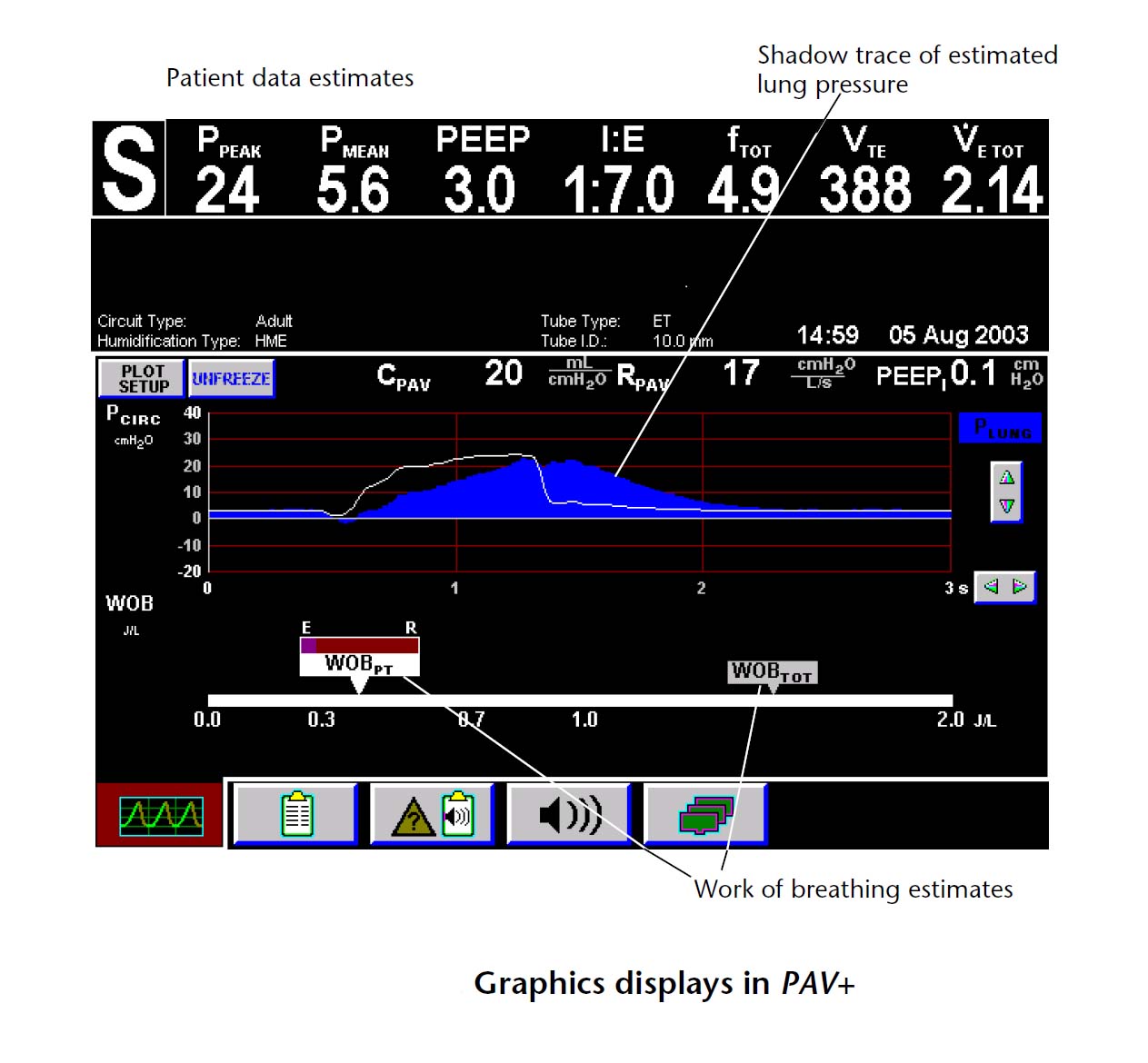
9)PAV
Because the characteristic of PAV of PB840 does a compliance and resistance at the automatic-gaging
It is in not setting a direct flow gain and a volume gain like Evita of the Drager Inc. and becoming the form to set the auxiliary percentage of breathing work volume to with 5% of steps in 5-95% of ranges.
But, for its purpose, the thickness of the tracheal tube, the tracheotomia, or the cannulation, the capacity of the heating humidifier must be entered beforehand first first.
The algorithm which does a compliance and resistance at the automatic-gaging is as follows.
PAV (the ventilation) that PIP was incorporated into the end of the end-of-suction by 4 pieces of continuation as the startup is done and measures a compliance and resistance (It fixes a known value by the factor except the patient in the thickness of IBW and the tracheal tube, the tracheotomia, or the cannulation, the capacity of the heating humidifier).
Moreover, by the equalization processing by which the latest dater is set in the weight, it is improving the reliability of the measured value.
After that, it is adaptable to PAV according to the (setting) % help percentage.
After the startup ends, randomly, in once, it incorporates PIP into PAV (the ventilation) and it is measuring a compliance and resistance to 4-10 breathing.
During PAV ventilation, the graph of the airway pressure and the estimated intrapulmonary-pressure of the measurement, and breathing work volume and total breathing work volume of the patient are displayed by the bargraph at the graphic display.
(Figure ; Setting screen of PAV)
For the details of the arithmetic expression, because a various manual is exhibited to the home page at the PB head office, it should refer to this.
10)NeoMode
PB840 has the object weight of equal to or more than 3.5 Kg but equal to or more than 0.5 Kg and adaptable weight are extended when incorporating NeoMode.
The possible range of the setting of the side of the expiration, too, becomes able to be set to breathing number of times 1-150BPM, float rigger sensitivity 0.1-10LPM, 5-315 ml of taking air quantities of ventilation, intake flow 1-30LPM ż.
The mode can use all except TC.
NeoMode boils only a float rigger and becomes.
The base flow is trigger sensitivity + 1.5LPM.
It uses the following specification circuit and the filter and so on to show a performance.
When starting up NeoMode, SST(Short Self Test) must be always enforced.
The compliance and the resistance value of the patient circuit are measured by this operation and are used for the ironhand "NO" index.
ü@
The patient circuit :
Ventilator breathing circuit, neonatal,disposable (DAR)307/6922
Ventilator breathing circuit, neonatal,disposable, 4 feet (Allegiance HealthcareCorporation)7441-4S2
The filter of the side of the expiration :
Expiratory bacteria filter (DAR), disposable DAR part number 351P19005
Expiratory bacteria filter reusable, 22-mmISO (Neo Re/x800) 4-076407-00
The others :
Inspiratory bacteria filter, 22-mm ISOconnectors, disposable (D/Flex )4-074601-00
Mounting plate* 4-076405-00
ü@
11)TC
TC is the function to reduce breathing work volume which is caused by the resistance of the tracheal tube by the abbreviation of Tube Compensation.
This applies the assist feature of PAV to the tracheal tube resistance only by the application of PAV.
The reducing work volume can be set in 10-100% of ranges.
It is possible to use only by the spontaneous-respiration mode.
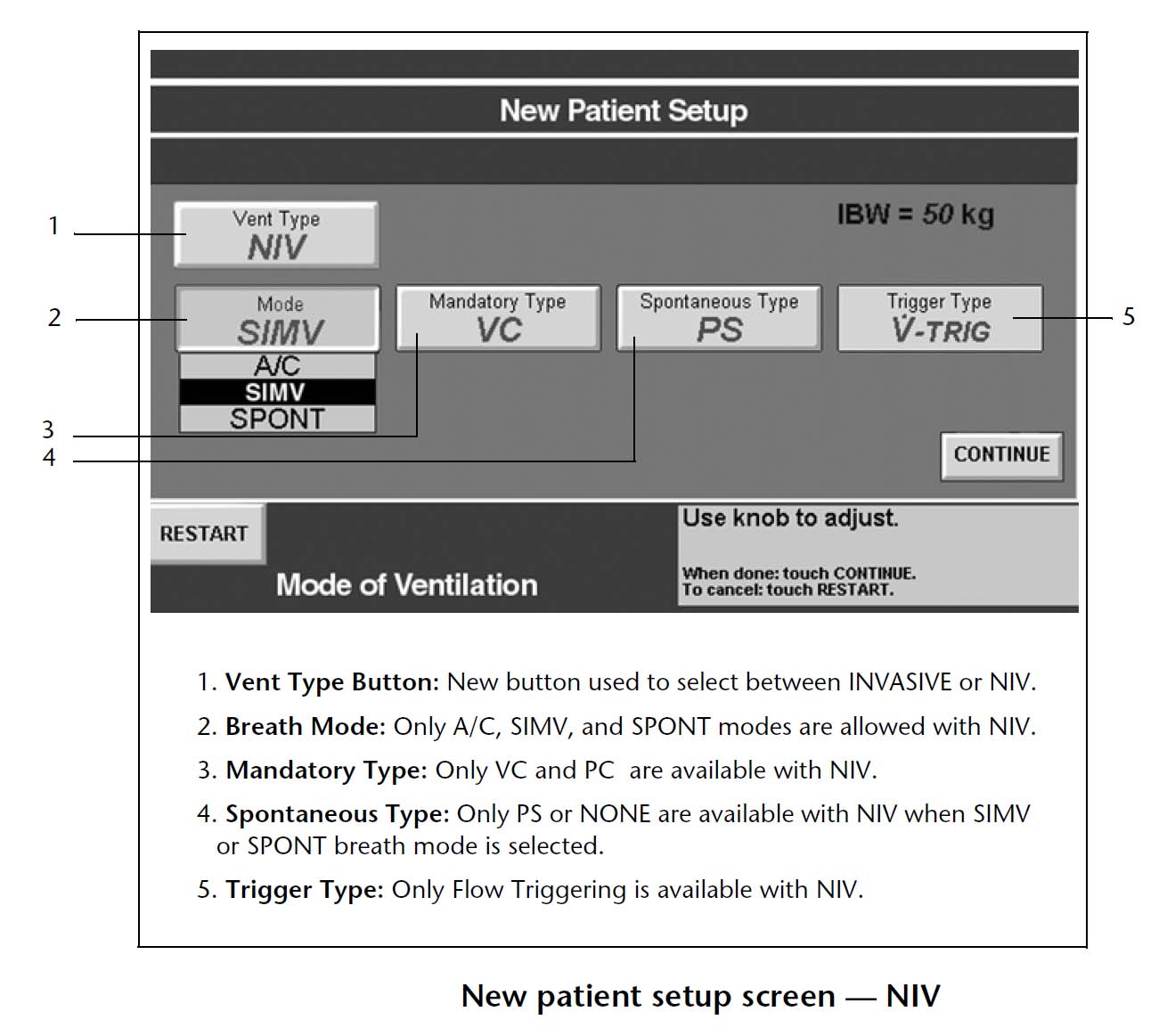
11)NIV
NIV is a low invasion positive pressure ventilation option by the mask ventilation which is called NPPV generally.
NeoMode however, it is possible to use and Nasal CPAP, too, becomes possible.
It does the operation to have supported a leak when operating NIV.
Following Mask is guaranteed in the operation.
ü@
Full-face Mask: Puritan Bennett® Benefit Non-vented Full Face Mask (large
, part number 4-005253-00), ResMed Mirage Nonvented Full Face Mask (medium)
Nasal Mask: ResMed Ultra Mirage Non-vented Mask (medium)
Infant Nasal Prongs: Sherwood Davis & Geck Argyle®
CPAP Nasal Cannula (small), Hudson RCI® Infant Nasal CPAP System(No. 3)
Uncuffed neonatal ET tube: Mallinckrodt Uncuffed Tracheal
Tube, Murphy (3.0 mm)
ü@
12) Battery drive
It is possible that to do 30 minutes of minimum operates by built-in battery.
13) The anaerosis back-up
It is valid in all breathing modes.
The oxygen concentration, breathing number of times, the taking air quantity of ventilation, the intake gas flow rate, the ventilating-pressure, equal "WO" in anaerosis back-up ventilation can be set.
The anaerosis back-up is automatically canceled when it pushes RESET key or the patient does a trigger continuously twice and the expiration air quantity of ventilation reaches equal to or more than 50% of the æŚ gas volume and it returns to the original mode.
In the SIMV mode, an active-ventilation is sent once after the anaerosis time passes and moreover it is the time when the anaerosis time passed and it enters back-up ventilation.
14)Dsens
The alarm sounds when detecting the miss of the patient circuit.
A difference between the æŚ gas volume and the expiration quantity of the resuscitator is compared.
It does a caution if the % value with loss quantity to the æŚ gas volume becomes above the set value.
15) 100% of oxygen keys
At the same time as oxygen is supplied to the patient for 2 minutes, the proofreading of O'2 senser ü[ is done.
16) The manual ventilation
The active-ventilation is æŚŗCed when pushing a manual ventilation key but is detecting expiration so as not for the patient to æŚŗC an active-ventilation in the expiration.
Until it passes for 200 ms from the beginning of the expiration, the expiration gas flow rate is equal to or less than 50% or 0.5 in the peak An active-ventilation isn't æŚŗCed until it becomes below LPM or 5 seconds lapse when still exceeding 50%.
17) The safety system
To prevent from operating system trouble, it is checking both of the control electronics and the gas circuit continuously.
This is called a background check.
In the MPU system, it prepares more extraordinarily and it is monitoring the operation status and the power failure trouble of the software using the hardware circuit in addition to the top of the software.
The Watch Dog Time-out circuit, the BUS Time Time-out circuit, the Built-in CPU monitor circuit, however, it resets a system once more to this, executing POST(Power On Self Test) at the extraordinary time, being.
It becomes the alarm condition of the malfunction when operating three times to 24 hours.
6. The operating
method
1) The basic operation
The setting operation uses the lower part screen.
It becomes the operation system of the touch screen method.
The basics choose an item by "the touch", and turn a control and enter and it fixes value with "the entry key".
The undo feature to return the set value before change works when pressing "cancellation" on the entry way.
The setting item has 4 items of "the ventilation setting", "the anaerosis (the back-up) setting", "the alarm setting", "the other screen".
Each Menu screen is displayed when touching being "DUREKA" with 4 items whichever screen it is.
It turns a control and it chooses and it fixes an item and value with "the entry key".
Because an operation guide is displayed on the screen, the operation is easy-to-understand.
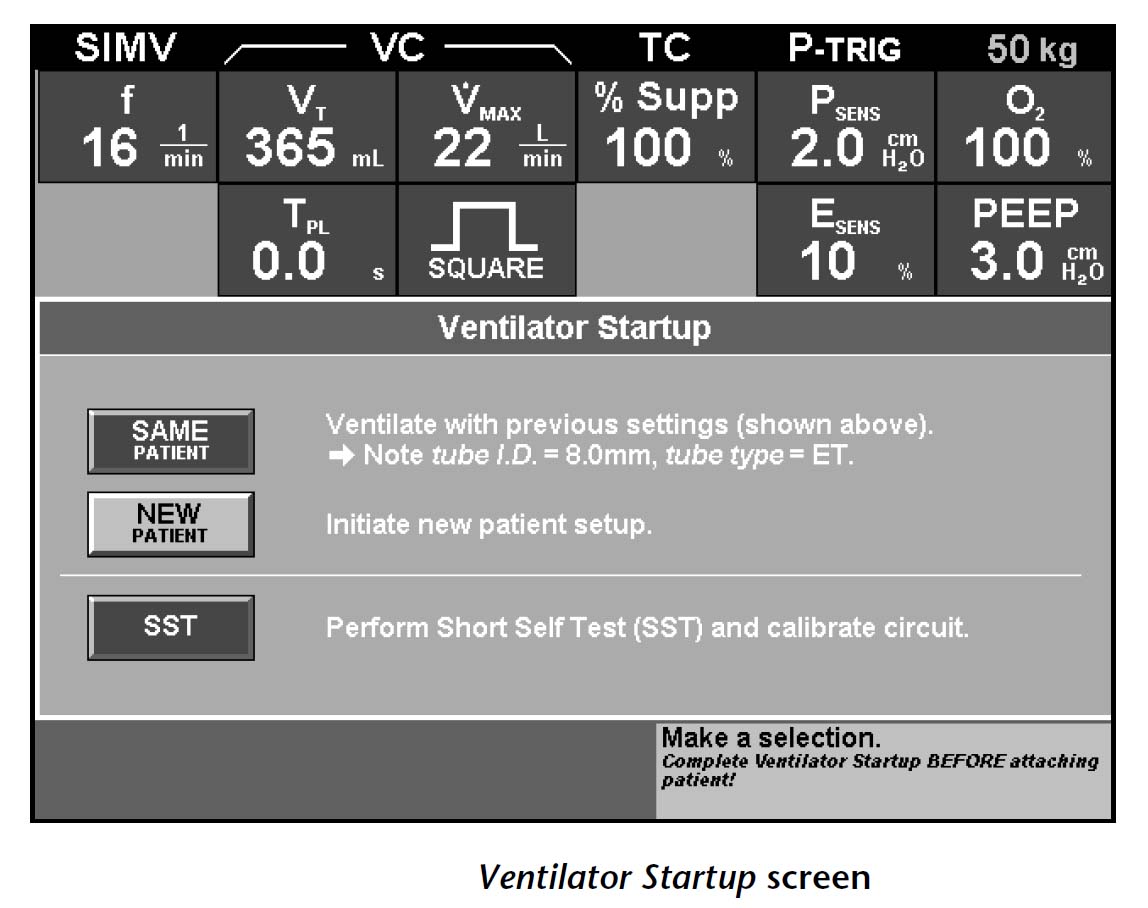
The start screen appears when making a power on.
If being the setting which is the same as the last time, it touches "the patient".
When choosing "the new patient", it becomes IBW entry screen.
It touches "IBW", and it makes IBW input-state, it turns a knob and it enters weight.
Next, it touches "continuation" and it moves to the next screen (the setting screen).
Because the set value of the mode (A/C, SIMV, voluntary), active-ventilation type (PV,VC,VC+), spontaneous-respiration type (PSV,PAV,BiLevel), the trigger type (the pressure trigger, the float rigger) appears, it touches, and it turns a knob to the button to hope for the change and it chooses it.
The other item, too, is displayed when touching "continuation" and moving to the next screen.
It chooses in the same way by the touch and the value types in by the turn.
It touches "to be fixed" if all setting ends.
It pushes "the entry key" last and it ends setting.
The normal ventilation starts when connecting to the patient.
After that, because the setting screen of the anaerosis back-up ventilation appears, it changes value if necessary, it touches "to be fixed" and it presses "the entry key".
The start screen can be begun from the beginning by touching to "the restart" at any time if being before pushing "the entry key".
When wanting to change set values such as the taking air quantity of ventilation and the air changes per hour while operating, it is possible to change in touching and choosing the item to hope for, and turning and entering a knob in the value, and pushing "the entry key" and being fixed.
(1)
Because 3 items of A/C, SIMV, the spontaneous-respiration are displayed when pressing the oddity of the ventilation mode and moreover " ventilation, it turns and it chooses and it fixes a control with "the entry key".
It presses "a next screen" and it sets a trigger formula, the kind of the active-ventilation and so on according to the screen-display in order.
(2) The setting of anaerosis back-up ventilation touches "an anaerosis" and it
sets to the anaerosis ventilation setting screen in the entering.
(3)
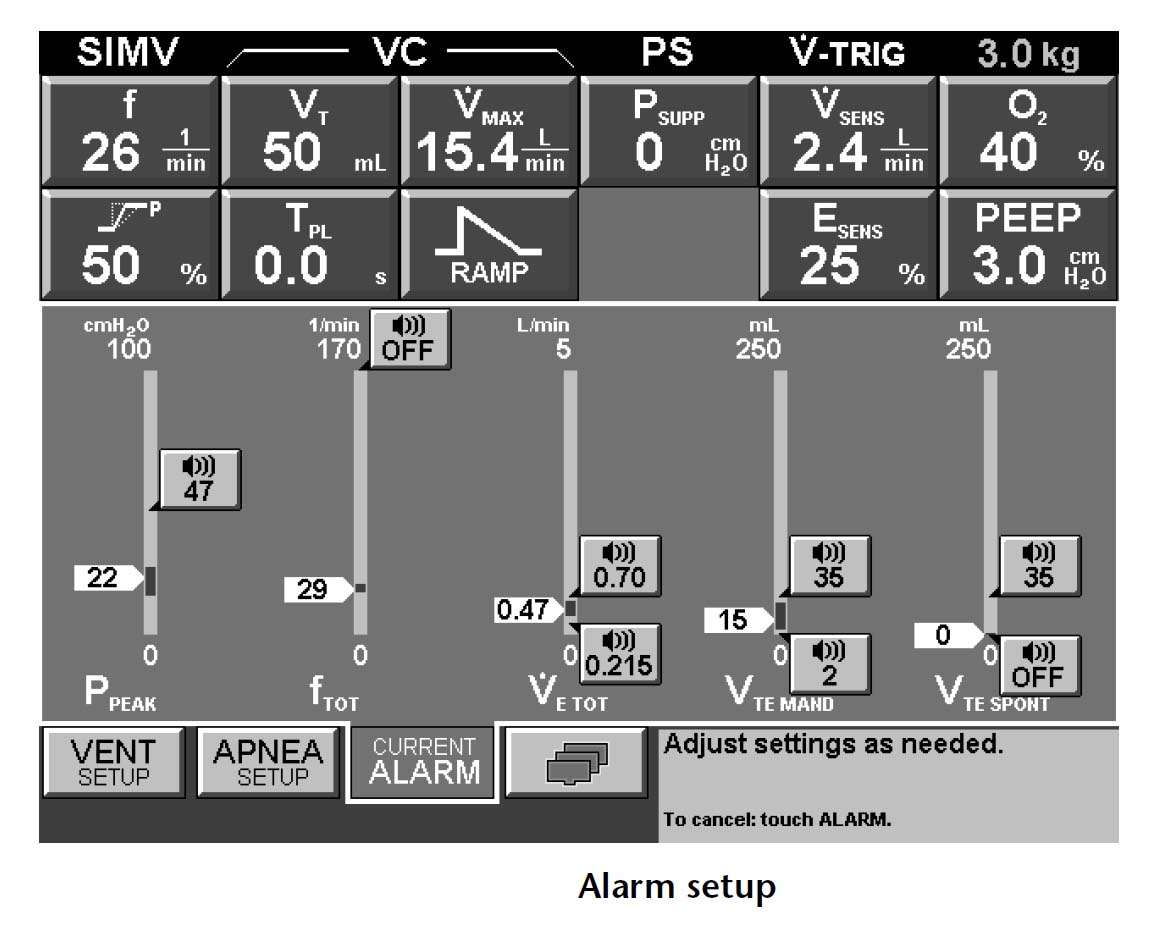
The setting of an alarm is entering "RU" in the alarm setting screen, touching "the alarm setting" which is displayed by the logo of the alarm.
(
Figure ; Alarm setting screen)
It touches and it chooses the upper limit of the alarm, the item to want to set because a minimum is displayed on the bargraph, it enters an alarm value with the control and it fixes it with "the entry key".
It is easy-to-understand visually because the upper limit of the bargraph or the minimum arrow changes according to the chosen value.
(4) The other
item
To change heating humidifier type, ü[ O'2 senser on, Esens, Dsens "NADO", it pushes and it sets the other screen button (this, too, is shown in the symbol-chart).
7. The monitor, the alarm
function
1) The outline
It is expressed in 4 steps of the high priority, in the priority, the low priority, the normal-system-operation.
Even if abnormal circumstances are canceled, it lights up an indicater until it resets it.
An alarm message is displayed at the upper part screen.
The alarm message consists of the base message, the analysis message, the disposal message.
The record of the alarm is recorded and the contents can be displayed when touching the alarm record button of the upper part screen.
2) The alarm item
The anaerosis time (20 seconds of original values), the circuit internal pressure upper limit (original value .60ćpH2O), the breathing number of times upper limit
(Original value off) , The taking air quantity of ventilation upper limit (original value 8.7 x IBW), the compulsion taking air quantity of ventilation minimum
(Original value 5.8 x IBW) , There are an expired volume per minute minimum (original value 0.0928 x IBW), an expired volume per minute upper limit (original value 0.1392 x IBW), a voluntary air quantity of ventilation minimum (original value 5.8 x IBW)
3) The equipment operation
It does a power decline, the abnormality of the equipment, a plumbing pressure decline, a transaction error in the
caution. At the equipment abnormality time, it becomes a relief valve disengagedness and it releases a patient circuit
in the big worrying.
4) The abnormality of the patient circuit
a) The blockade of the circuit
It is checking whether or not there is not a blockade of the patient circuit in all cycles of æŚŗC continuously.
The alarm operates when detecting a blockade and displays elapsed time.
Until or, pass for 15 seconds until the inspiratory-pressure becomes below 5ćpH2O, it releases a relief valve.
After that, it repeats PCV of 2-second intake time inspiratory-pressure 15ćpH2O in the regular interval.
It returns to the original operation when blockade status is solved.
b) The connection fault of the circuit
Continuation's one with three times when not detecting a flow and pressure in the 200 first ms of the expiration
When Dsens becomes above the set value with the ventilation, when detecting the max-flow which doesn't reach a setting level in the maximum intake time at the time of PSV, it thinks as the miss of the circuit, the alarm operates and displays elapsed time.
It opens an exhalation-valve and it supplies 100% of oxygen 10LPM.
When a connection fault is canceled, it returns to the original operation.
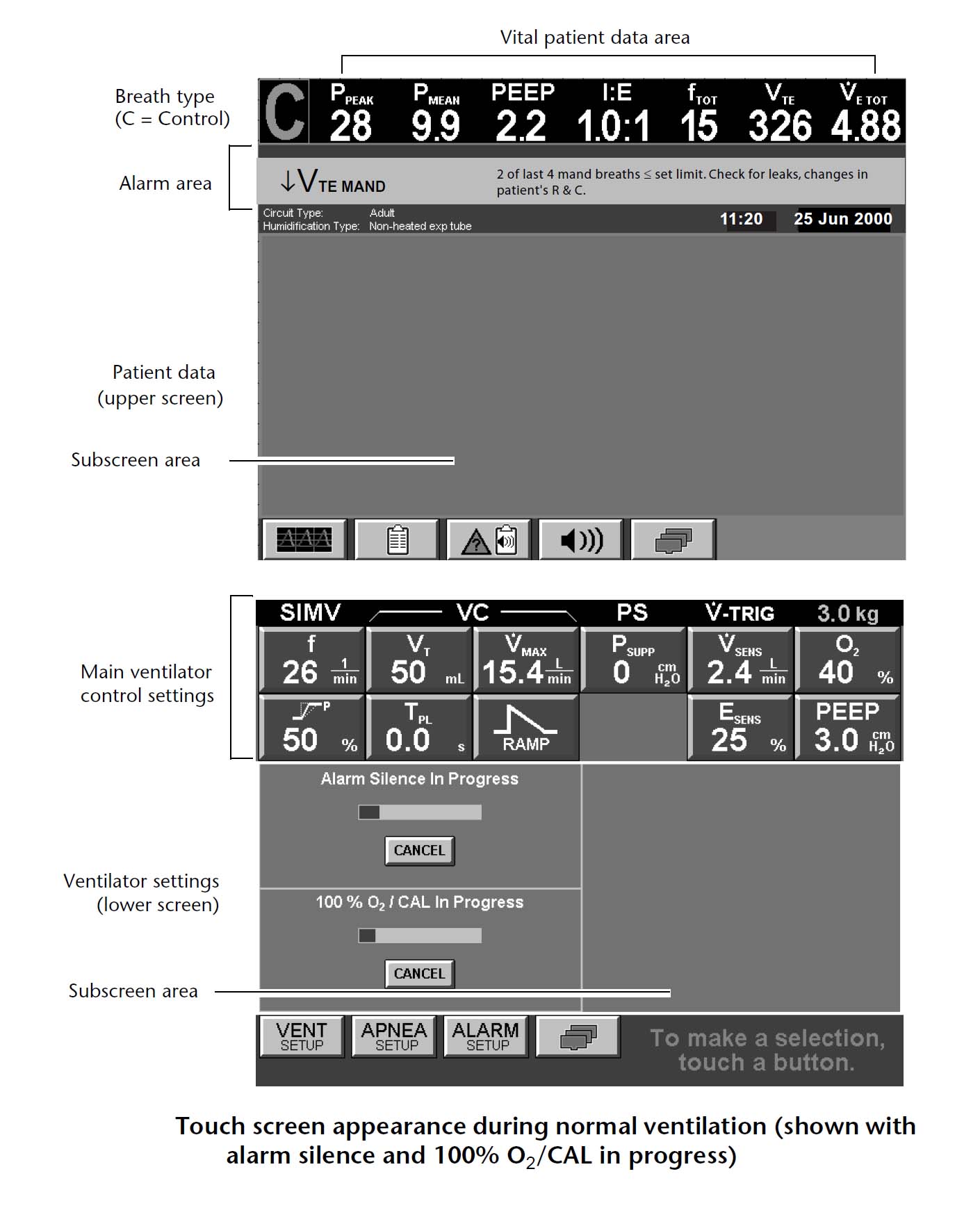
Setting is displayed at the lower part screen.
Patient information is displayed at the upper part screen.
As for the actual measurement of the air changes per hour, the airway pressure, the expired volume per minute and so on, value is displayed in the upper side of the upper part screen.
It displays an alarm message in the alarm area under it.
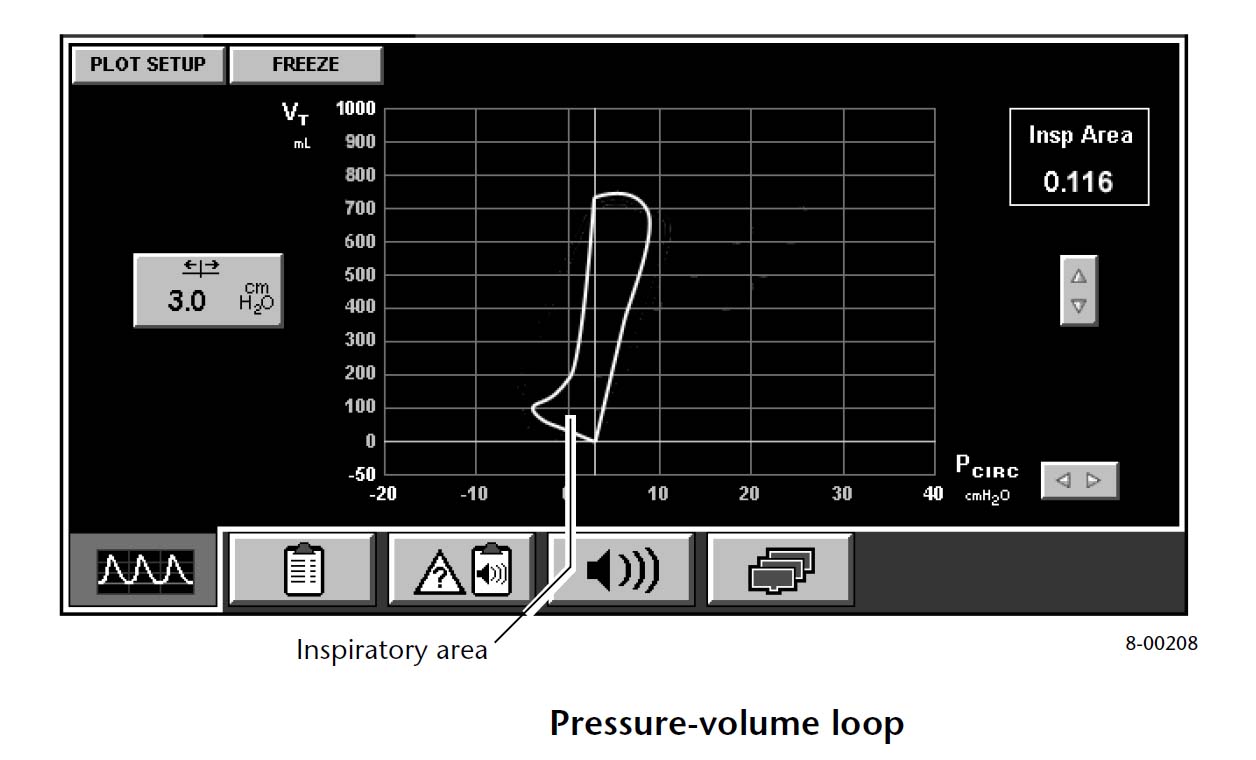
It puts on 2 corrugations with the graphic presentation out of the pressure, the flow, the quantity to the sub screen area.
Also, the pressure-the air quantity of ventilation curve, too, can be displayed.
It displays the record of the alarm by the key touch.
As for the humidifier, F&P is included as standard equipment.
10. The maintenance
1) The exhalation-valve
An exhalation-valve is had in this interior of the body and there is not need of the resolution, the wash, the sterilization in homely use.
There is a bacterial filter that a heating was made the front of the exhalation-valve and with this, the patient circuit is because it doesn't pollute.
Therefore, the circuit can be simply composed only with two tubes.
It is in the origin difficulty about mistaking a construction by the circuit after sterilization, too.
2) The filter
When there is a continuous running duty on the 15th, when expecting that the other resistance becomes big before commisioning, it does a test sequence by the SST and it confirms resistance.
As for air cleaner ü[, it confirms that the resistance is the range of 1-4ćpH2O/60LPM or 0.5-2ćpH2O/30LPM.
As for the expiration filter, the resistance is 0.6-2.4ćpH2O/60LPM or 0.3-1.2ćpH2O/30 It confirms that it is in the range of LPM.
After nebulizer use, it attends to this point more.
Incidentally, the bacterial filter can only be an autoclave.
It exchanges if sterilized every year or 100 times.
11. The regular
inspection
1) Every year
It does the proofreading of a transducer with all kinds by the service engineer, a test.
2) 2 every years
It exchanges an O'2 senser ü[ standing-next power back-up battery.
3) 10,000 hours
The service engineer exchanges parts with all kinds using the preventive maintenance kit by it.
12. The fault
1) There was a problem of the young coming to an end in the sales and the support and so on before but it solved becoming this to the direct sales of the Tyco Healthcare Inc..
The posture to the information disclosure, too, is improved and now, it gets for the downloading to be possible to the service manual in addition to the user's manual on the home page.
2) It compared an operation menu system to 7200 and it became and it was improved but the menu structure still has the room of the improvement.
It sometimes requires to push of the operation of being fixed later and moreover an entry key and it is felt as it is possible to operate immediately by the change, the entry and there is not system in the operation system.
Therefore, it isn't sometimes possible to complete not to see a guide display.
Moreover, there is a place not to agree with the accepted term, too, generally in the term which is displayed in Japanese and there is an unclear thing of the meaning, too.
For example, it isn't sometimes possible to understand what the term such as the setting, the continuation, the cancellation, the restart because the Japanese translation is bad (will have requested the general translator who doesn't know a resuscitator) means, too, Most (near this, too, was well improved).
3) The Japanese display is easy-to-understand and is popular specifically with the paramedical, but becomes Japanese more than necessary and there is a place where it is difficult to understand oppositely, too.
ÅŖæF, because it is a kanji=Chinese even if it is called Japanese, there is a place where mom of the English abbreviation is better, too.
4) An operation system is slightly confused because it will be the problem of being accustomed, but there is one which is unique, to be few and the grammar is different from the servo and Ebita.
It becomes anyhow if there is a guide by Japanese and it follows to that but if saying an ideal, it should think of the operation system which anyone can understand even if it doesn't guide.
5) It is possible to evaluate that the exchange of the patient circuit became easily with the filter in front of the exhalation-valve but the one with the unnecessary running cost which takes only about the part is negative.
6) It is wonderful to become the performance which is equal to Servo i with a newborn baby feature extended by NeoMode but that the test sequence must be done to change to NeoMode is troublesome.
7) That the graphic display puts on only 2 corrugations by the simultaneous display is inconvenient. That the pulmonary
mechanics screen, too, can display only PV curve is enough.
8) As for the performance, as the resuscitator of the summit level, that there is not a problem but that the thing except the feature which was developed by the other company doesn't have an original mode and a feature at all lack abilities as the leading company.
ü@
Puritan Bennett 760, 740
Bennett As for 760,740, the air plumbing operates with the resuscitator of the piston drive system even if it is not.
In the active-ventilation, it makes 150LPM and PSV makes a maximum intake flow rate, 300LPM, possible with the friction recipes ton and the powerful drive-mechanism.
With the product which supports widely from the conveyance business to ICU, it is the concept which is the same as T-Bird (the Bird Inc.).
It operates for 9 hours if using the outside battery, too, for 2.5 hours with built-in battery.
760 and 740 big differences are about whether or not it has PCV mode.
Moreover, at 740, start-up speed setting by PCV, PSV of the active-ventilation, the Flow Cycle setting of PSV, an intake pose, an expiration pose, too, are omitted.
The model number becomes in łß with the difference of the option.
ü@
2. The
performance
1) The mode that it is possible to use
A/C
SIMV + PSV
PSV
---------------------------------
Flow trigger
PCV (Only 760)
+PEEP
2) This proximal dater
The maximum intake gas flow rate
The active-ventilation
.150LPM
PSV. .300LPM
The number of the maximum
active-ventilations 70BPM
The maximum SIMV number of
times .70BPM
The battery drive time Built-in battery ;
2.5 hours
The battery of the outside of the option ; About 9 hours
3. The control circuit, the
controlling mechanism
The use of the resuscitator of the conventional piston drive system was limited to the field which doesn't need high efficiency for the anesthesia and the home, and so on, because of the inertia and the friction of the piston, the weakness of the drive-mechanism, which late the response.
On the other hand, there was an agreement to make to make a quick response and a high maximal flow possible but that the gas drive system is necessary in the air plumbing on the principle.
Also, the trouble which is related to the air plumbing, too, is "TUTA" in the troublesome problem.
T-Bird which used a turbine from the Bird Inc. as the answer to these appeared but the Bennett Inc. opposes by the friction recipes ton that the piston doesn't touch an intercylinder wall absolutely.
(bigin pressure drop which depends on the ventilation condition in the response time according to the company data but is about 80-100 ms
- back to baseline )
Bear of this to be said to that it does ŚLłė"NI"ÆZ"KU" and, that it is more excellent than 900 C and 8400STi of 1000 and SV300, Evita It is equal to 2.
Also, it is possible to foresee that the control system is excellent in the obedient one about the pressure corrugation, too.
2) The characteristic of the mechanical mechanism
The patient circuit is two simple tubes of the Bennett style and an exhalation-valve and Fluothane Sir are protected by the heating filter.
The trigger mechanism is a flow trigger formula.
3) The gas flow rate measurement
It measures an expiration gas flow rate with the sensor of the delta-pressure type. The intake gas flow rate doesn't have
but calculates a sensor from the amount of transfer and the piston internal pressure of the piston.
4) The friction recipes ton
It is the friction recipes ton that is equivalent to the intake valve.
There is a crack (50 micrometers) of the hair 1 business between the piston and the cylinder and the leak occurs continuously.
Because the amount of leak and the piston internal pressure have constant relation, if measuring a piston internal pressure, the amount of leak can be estimated based on the known quantity which is recorded to the ROM.
The piston control system is operating to revise a leak.
5) The expiration valve
It is the method which changes the pressure which is composed of PEEP pump and the inspiratory-pressure which occurs with the piston by Solenoid-controlled valve and drives a balloon valve.
If the PEEP pressure declines in the patient circuit leak and so on, to maintain PEEP, a piston is driven.
However, there is not a mechanism to make fall to actively even if the PEEP pressure rises with expiration gas.
The O2The dense fog (equal to or more than 35 psi) which was entered from the plumbing is decompressed with the filter, the non-return valve, the regulator.
Decompressed oxygen and fresh air are 150 with the beginning of the expiration of the patient It is inhaled at the speed of LPM.
An one way valve is provided for the entrance of the piston.
Mixing Manifold uses two kinds of O2 solenoids in case of inhalation operation, and controls the time which jets out oxygen to the intercylinder and fixes an oxygen concentration.
After the expiratory-phase begins, even if it is late, in 0.8 seconds (the piston capacity is 2 being 2/150 minutes=0.8 seconds because it is large), the induction stroke ends and preparations of the trigger detection are complete.
After that, to maintain baseline pressure, the piston begins an emission.
The piston control system works to accompany the operation of the trigger, for PSV or the active-ventilation to begin and to maintain pressure and a flow rate.
Gas in the piston becomes the inspired-gas of the patient via the one way valve, O'2 senser ü[ and the relief valve (relieving at the time of the abnormal fluid pressure).
Expiration gas from the patient is emitted in the course of the heating filter, the exhalation-valve, the expiration gas flow rate sensor.
In case of the expiration, it is closed at the pressure to have made with PEEP pump but in case of intake, the exhalation-valve closes an exhalation-valve in the intake gas pressure.
These changes are done by Solenoid-controlled valve Exhalation solenoid.
As for the pressure sensor, zero point proofreading is automatically done by autozero solenoid.
5. The control
software
1) The trigger formula
In the flow trigger formula, it is 1-20 It is possible to set in the range of LPM.
The piston internal pressure declines when the patient begins intake but a piston action is controlled to maintain baseline (PEEP/CPAP) pressure.
The movement of the piston is measured in the rotary encoder but the trigger operates when the measuring quantity exceeds flow sensitivity.
2)A/C
Usual active-ventilation and the same When depending on the maximum pressure limit, intake ends
immediately. The taking air quantity of ventilation is 40-2,000 ml.
3)SIMV
The trigger window is 60% of the SIMV cycle time in the fixed time method.
If the expiration gas flow rate doesn't become equal to or less than 30% of the peak rate of flow so as not for breathing to overlap, the following active-ventilation doesn't start.
4)PSV
The intake flow rate is the following of 10LPM or the one of the peak rate of flow to the end-of-suction end recognition condition.
When declining from equal to or less than 25% of being "DURE" or more few values, when rising above 3ćpH2O from the PSV set-pressure, when intake in equal to or more than 3.5 seconds continues (being 2.5 seconds at the circuit for the infant), being "DUREKA" which is is used.
But, within 300 ms, it becomes the case where this condition lasted for equal to or more than 100 ms from the beginning of PSV.
Incidentally, in the maximum intake time, it is limited to 5 seconds.
For the capacity of the piston to be agreed, equal to or more than 2,000 ml of continued intake are impossible.
5) Battery drive
It is possible to drive for about 9 hours if using a battery of the outside of the option for 2.5 hours with built-in battery.
If not needing the addition of oxygen, the oxygen plumbing is unnecessary.
6) The anaerosis back-up
It operates if there is an anaerosis for 20 seconds in the validity only in the spontaneous-respiration mode.
It sets an anaerosis parameter because "the anaerosis mode setting key" lights up and breathing number of times, the taking air quantity of ventilation, the flow rate key blink when choosing a spontaneous-respiration mode.
An anaerosis back-up is canceled when it pushes RESET key or the patient does a trigger continuously twice.
6. The operating
method
After choosing an item, pushing the button, it turns a knob and it sets value, and it pushes and it fixes an entry key.
7. The monitor, the alarm
function
1) The alarm condition
It is expressed in 3 steps of the alarm, note, the normal-system-operation.
Only the lamp of note lights up when abnormal circumstances are canceled.
The alarm item includes the breathing number of times upper limit, the taking air quantity of ventilation upper limit, a taking air quantity of ventilation minimum, a low inspiratory-pressure, the circuit internal pressure upper limit, an expired volume per minute minimum.
The alarm contents of the top priority are displayed in the message window.
The panel left side displays an airway pressure, a breathing rate, a taking air quantity of ventilation, an expired volume per minute, an equal "WO" monitor in the monitor part.
8. The display feature
That the airway pressure is the bargraph of the LED is displayed at the value. Currently,
it isn't possible to do a corrugated display.
As for the humidifier, the cascade I type is included as standard equipment but F&P, too, can be chosen.
10. The maintenance
1) The exhalation-valve
An exhalation-valve is had in this interior of the body and there is not need of the resolution, the wash, the sterilization in homely use.
There is a bacterial filter that a heating was made the front of the exhalation-valve and with this, the patient circuit is because it doesn't pollute.
Therefore, the circuit can be simply composed only with two tubes.
It is in the origin difficulty about mistaking a construction by the circuit after sterilization, too.
2) The filter
As for the bacterial filter of the exhalation-valve, the resistance is 4cmH.2It confirms that it is the following of O/100LPM sometimes.
After nebulizer use, it attends to this point more.
Incidentally, the bacterial filter can only be an autoclave.
11. The regular
inspection
1) The filter
It exchanges the bacterial filter (the nebulizer circuit, the pressure monitor circuit in front of expiration Fluothane Sir in front of the heating humidifier) of 4 ēė in amount within 3,000-5,000 hours.
2) The others
Besides, it does various "HUANHUIRUTA-", the exchange, the wash of the bacterial filter to the instruction of the manual.
12. The fault
1) The big intake which exceeds 2 liters and the extreme tachypn ea can not be supported.
2) Because the piston inhalation time is necessary, after suction operation, and so on, there is possibility that enough PSV can not be provided.
ü@
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}