Drager
Evita XL,Evita4
In EVT-800 of the cheap-edition which limited EVT-1000 in 1985 to the basic function in 1990 as the beginning, in 1993, EVT-880 was sold in EVT-2000(Evita 2) and in 1992 of the minor change version and in 1995, EVT-4000(Evita 4) was sold.
In EVT-2200(Evita2 Dura) which simplified the graphic function of EVT-4000 in 1997 and lowered a cost, in 2004, EvitaXL which reinforced the graphic function and the operation system of EVT-4000 was sold and the feature of SmartCare and Low Flow PV Loop "NADO" was added.
Evita utilized BIPAP which is the product of the exhalation-valve control technique which is excellent with the artificial respiration machine which possesses cutting-edge hard and software at the same time and AutoFlow, an intake flow technology.
Pressure Limited Ventilation (the P max control), increased pressure speed variable (slope control of pressure rise), it was excellent.
It is fully loaded with the various features of "NADONO" that PTV of the newborn baby (equal to or more than 500 g), too, becomes possible when having to be applicable and moreover NeoFlow of the option from the adult area (the equal to or more than 15-kg weight) by the large-sized electrochromatic display touchpanel the trigger sensitivity of the highest level by the sensing technology, the interface by it, to the infant area (the equal to or more than 3-kg weight).
Software is continuously improved and currently, SW6.0 is the most new version.
2. The
performance
1) The mode that it is possible to use
CMVźIPPV(=A/C)
ASB (=PSV)
SIMV +ASB
EMMV +ASB
BIPAP +ASB
APRV
+PLV(pressure limited ventilation)
+PEEP
+Intermittent PEEP
+Apnea ventilation
+AutoFlow
+slope control of pressure rise
2) This proximal dater
It is 120 during the gas supply system źźźźźź early stage flow rate of a maximum of 8 ms LPM.
The maximum intake gas flow rate
Active-ventilation źźźźźźźźźźźź120LPM
ASB źźźźźźźźźźźźźź180LPM
Intake gas slew-rate źźźźźźź250L/s2ü@ü@ü@
The number źźźźźź100BPM of the maximum active-ventilations
The maximum SIMV number of times źźźź100BPM
ü@
3. The control circuit, the
controlling mechanism
1) The outline of the controlling mechanism
Evita connects each with each unit of control unit, electronics, pneumatics in CAN bus (the communication speed of 1MBit/s) with the resuscitator of the computer-control equipped with MPU (68332 a of Motorola).
It is equipped with special MPU to the display, too.
It is equipped with 3.5Mbyte Flash EPROM and 1.5MBite RAM to the memory.
2) The characteristic of the mechanical mechanism
The new Mattick circuit is standard but the directions of the sensor have a characteristic.
It adopts the mechanism which makes to do the can to proofread which as automatic and moreover it used a pressure transducer and an oxygen concentration sensor, Fluothane Sir to the patient.
Therefore, the stable sensing where there are few age softenings becomes possible.
3) The gas flow rate measurement
(a) The
side of
intake
It calculates an intake flow rate and intake quantity from the pressure information in the place around the flow control valve and the positional-information of the flow control valve.
(b) The
side of
the
expiration
An expiration gas flow rate is measured with the flow transducer of heat ray type "hot wire".
This becomes disposable but if not considering sterilization, the continuous running duty, too, is possible.
0 proofreading of this sensor is done when there is not a flow in the inspiratory-phase.
An air quantity of ventilation is processed in "DEZITARUHUIRUTA-" (2nd.transversal & 4th.bessel filter) after an analog to digital conversion is done.
The equalization of the expired volume per minute is done by this and brings about the characteristic which is near the 1-minute accumulation.
(It is used as the PEEP compensation information of the exhalation-valve, too, but) being general, the alarm is special and the measured data ü[ of the expiration expired volume per minute are independent with the machine control type.
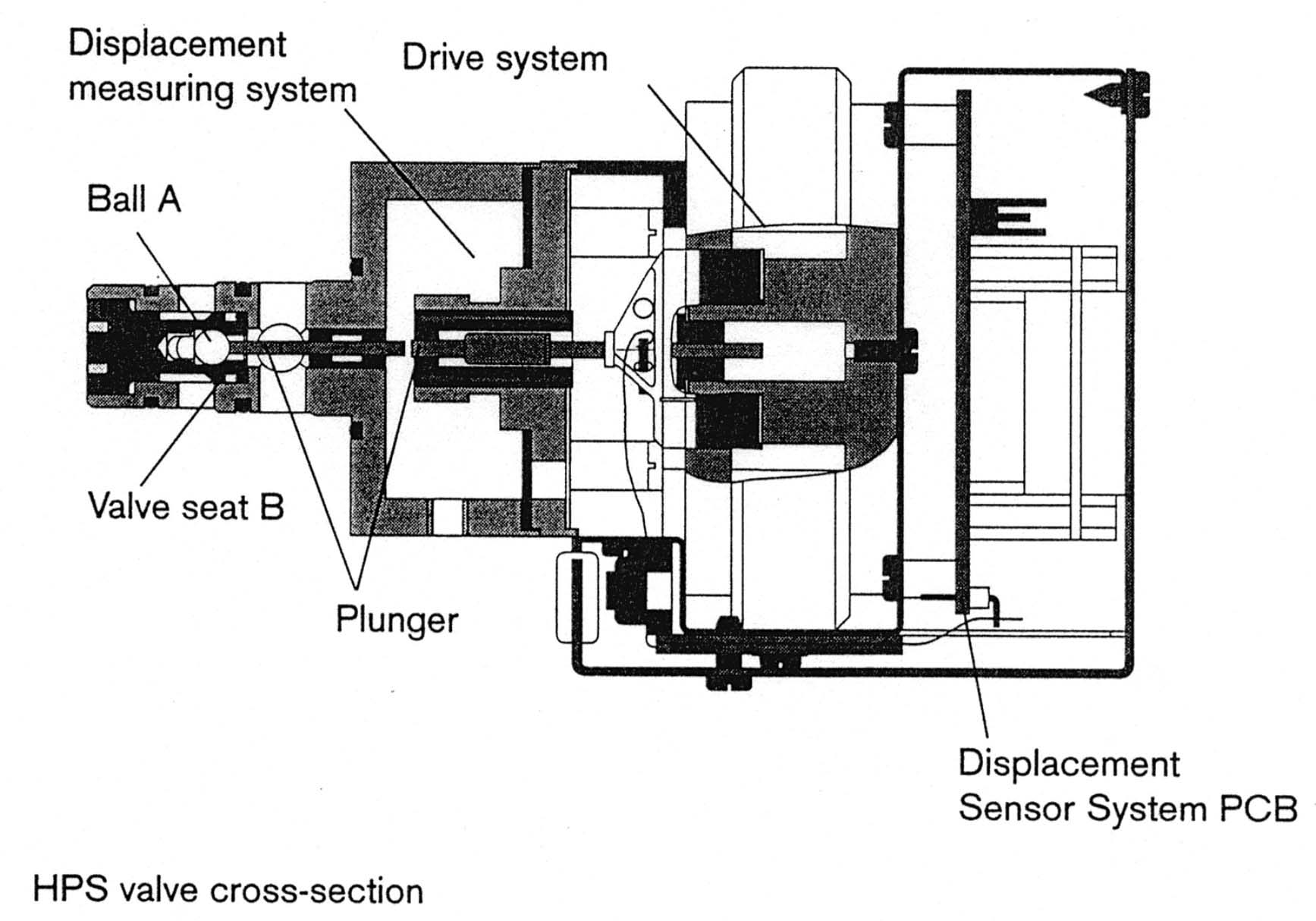
An intake valve (Y8, Y9 of the new Mattick figure) is called HPSV(High Pressure Servo Valve) but this is driven in the principle like the electromagnetic coil which drives a speaker for the music.
It does an intake valve drive circuit to the servo control by the digital circuit based on the pressure and the flow rate information.
The handling was easy, but the structure was complicated, there was weight and the exhalation-valve unit of the removability of EVT-1000 was expensive.
After EVT-2000, it was improved in the small, light-weight and simple structure and it became inexpensive consequently.
The expiration valve is a diaphragm valve but this drive gas generator Ź\ consists of the digital circuit which controls the PEEP controller (Y2 of the new Mattick figure) which the electromagnetic coil can adjust to the optional pressure and this.
The drive electric current can adjust PEEP controller valve to the optional gas flow rate with the valve which does HPSV and a similar feature.
It makes an exhalation-valve driving-pressure for the purpose(= PEEP driving-pressure) with releasing the quantity which is optional more than the drive gas which passed through resistance R2 in the big worrying.
The exhalation-valve driving-pressure is adjustable based on the information and the expiration gas flow rate information on the pressure sensor on the side of the expiration digital-ly.
Specifically, in case of BIPAP operation, the exhalation-valve drive-system shares the role which is equal to the side of intake.
The gas of O2/Air supplies circuit drive gas via decompression-valves DR1.1, DR1.2 after removing dust, moisture from the central plumbing with entry filters F1.1, F1.2.
It changes an drive gas source in Y1.1 to be using Air but for usual drive gas to be O2 when Air is blocked off and to secure circuit operation.
Y1.3 is the emergency-valve to miss the pressure which crossed an airway pressure alarm set value.
The pressure sensors S6.1, S6.2 of O2/Air are measuring pressure in flow control valve "HPSV"Y2.1, the Y2.2 eve.
Based on the data of these measured data and the airway pressure, flow control valves Y2.1, Y2.2 are doing the mixing of O2/Air and 2 pieces of duty of the control of flow like a lifetime.
Y3.1, D3.1, F3.1, D3.2 are the system which opens a patient circuit in the big worrying when the case of the machine failure and distributed-gas from the air plumbing is stopped.
Y1.2, Y3.2 are the system of O2 sensor S3.1 for the proofreading.
It supplies gas for the proofreading to Y3.3 at the same time as Y1.2 opens when pushing the proofreading key of the O2 sensor and opens Y3.2.
Y3.3 can pass proofreading dense fog while it does a gas supply to the patient and proofreading gas to the O2 sensor separately.
Need which opens a circuit to proofread an O2 sensor passed away because the proofreading became possible without mixing with the patient by gas during O2 sensor proofreading by this.
D3.3 is the relief valve (the relief valve) that the patient circuit assumes the situation which was made high-pressure extraordinarily.
Y1.4 supplies nebulizer drive gas.
Y6.1, Y6.2 are the proofreading valve of the airway pressure sensor, and by this operation, Y6.1, Y6.2 open each of airway pressure sensors s6.1, s6.2 in the big worrying and do zero proofreading.
P1, P2 are the port which is opened to the main unit front that it is possible to support when the option which measures a mouth-pressure and an esophageal-pressure and so on in future is developed in the addition (Unused at present).
s6.2 is Y4.1, and is watching over the expiration line pressure change at the usual time based on the pressure which is being made to occur and sends a trigger and a signal for the demand.
By the simplification of the circuit, it is doing exhalation-valve drive and PEEP adjustment with one valve Y4.1.
This PEEP/PIP valve is an electromagnetic driven valve and controls PEEP and the pressure (PIP ) of the high-pressure aspect of the BIPAP mode.
It is driving an exhalation-valve in the removable type exhalation-valve unit ("PE-SIENTOSISUTEMU") at the pressure which was made with this valve.
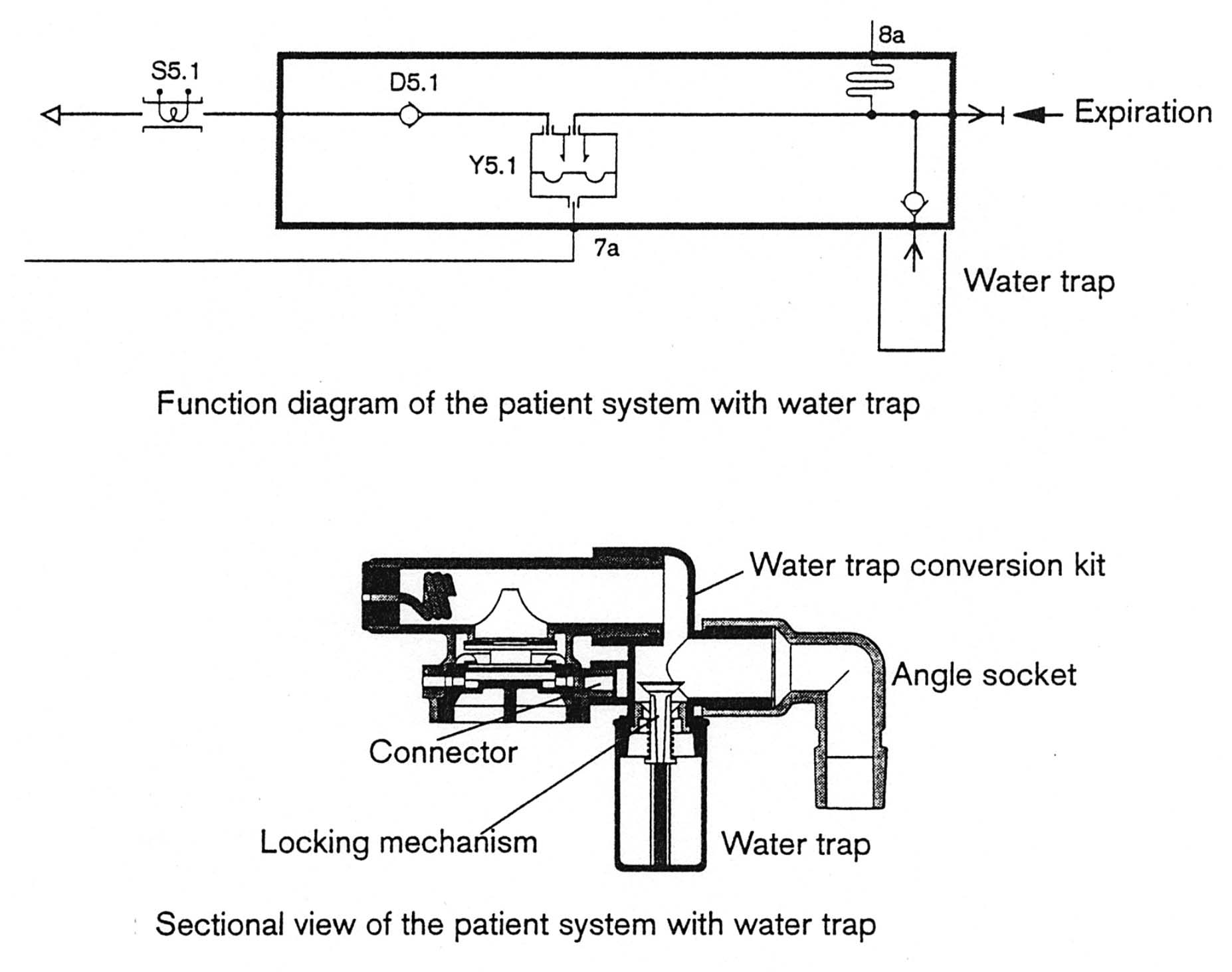
Rectifying an expiration style with the mesh board by S in "PE-SIENTOSISUTEMU"
S5.1 is "HURO-SENSA".
The proofreading of "HURO-SENSA" is controlled by the software and an expiration flow rate during the intake time is done during the time which is not.
It is to attache or remove an exhalation-valve unit (block "PE-SIENTOSISUTEMU" which Y5.1, D5.1, S, S5.1 are stored in) that Ebita's "NIYU-MATITUKU" circuit becomes a way of second dan repeating driving basically with of Solenoid-controlled valve ü© new Mattick.
A heat ray type is used for "HURO-SENSA" S5.1 of the expiration.
5. The control
software
1) The trigger formula
Evita has a characteristic to the pressure demand and the point which distinguishes between the trigger, being clear.
Evita4 since then, it opens intake flow valve (Y2.1,Y2.2) by the pressure demand which senses an exhalation-valve eve airway pressure change and it adopts the flow trigger formula to do in the trigger based on the then occurring flow rate.
A pressure trigger and all float riggers intermingle in EVT-1000 and EVT-2000 but in Evita4, they are unified by the float rigger.
It hardly feels the necessity which adjusts float rigger sensitivity but if necessary, the "Extra settings" key which is in the ventilation mode setting screen can be set among 0.3-15LPM by pushing it, too.
Even if it sets to 0.3LPM temporarily, Auto-Cycle does the operation which was as stable as that it doesn't happen almost.
Demand sensitivity is fixed on 0.2 mbar of delta.
The base flow doesn't lie in that it should be surprised.
According to the manufacturer, as for the basis which doesn't have a base flow, [when there is not the need] is described.
However, it is NeoFlow(BabyLog The one of the ventilator ability for the newborn baby who incorporates 8000 features just as it is.
Option. Fluothane Sir is BabyLog Because it is using a base flow at ) of installed between the Y peace tip and the tracheal tube in the one which is the same as 8000., it is estimated according to the inevitability which makes a delay the least and the difference with sensor itself.
At least, at the heat ray type sensor that external was done, it is because there is recognition that the possibility that the problem occurs to the precision maintenance and the reliability can not be fully excluded.
If there is not a base flow, it becomes for the float rigger to have been able to be processed only by the flow information on the side of intake.
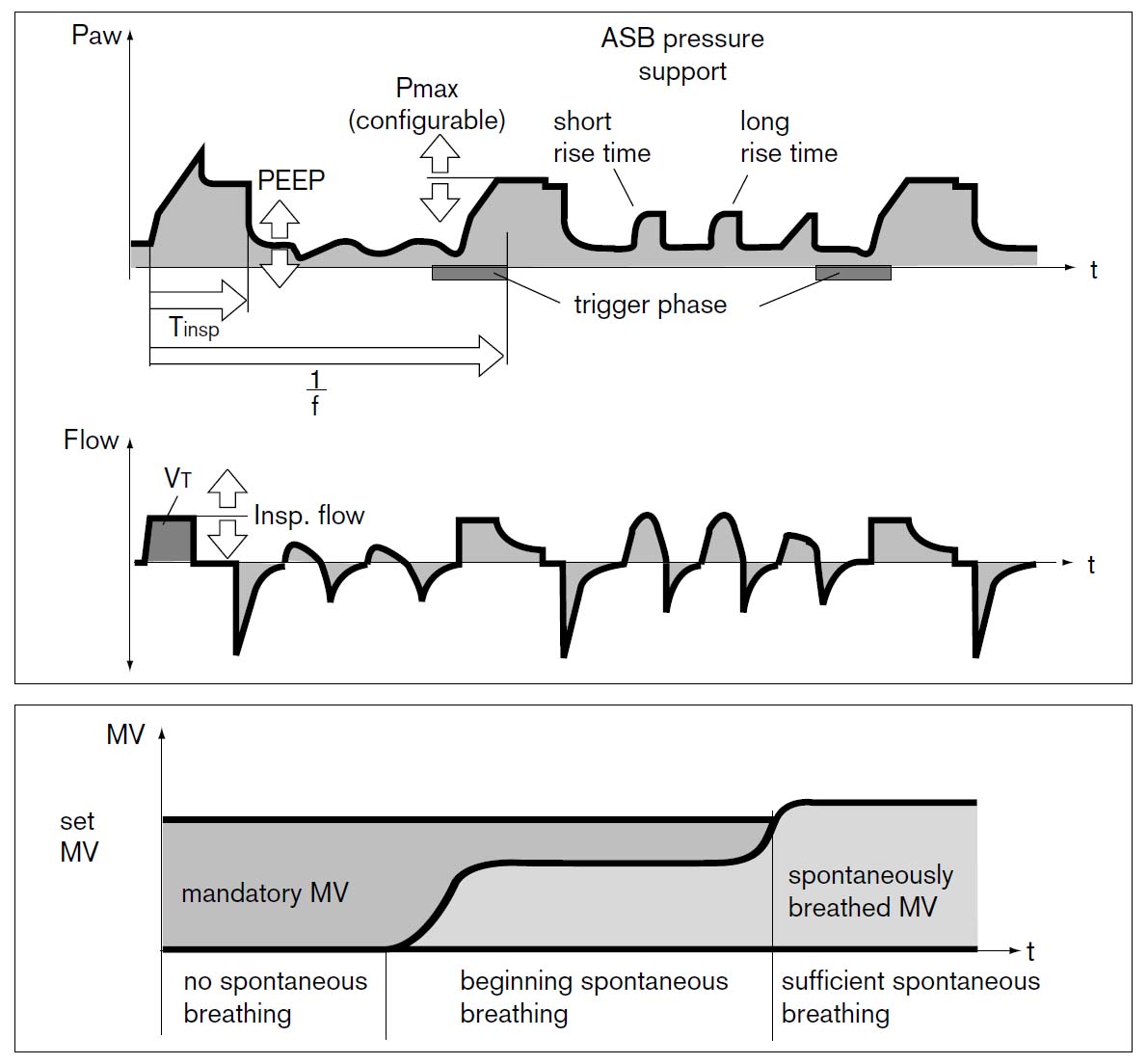
2) The increased pressure speed variableness (slope control of pressure rise)
It is possible to use by all pressure ventilation modes such as ASB, BIPAP, AutoFlow.
At the start-up time (the period of slope control) of intake, the standard pressure rises continuously with the passage of time.
An intake valve is done by the servo control for the inspiratory-pressure to consist of standard pressure within -0.6 mbar.
The increased pressure speed is variable in 64ms-the 2.0-s range.
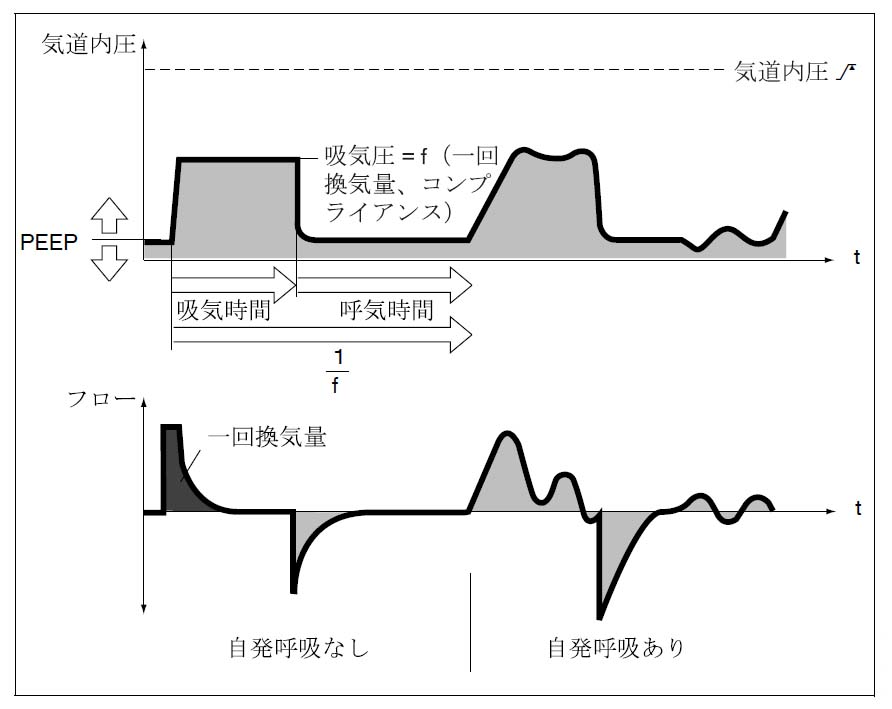
3)IPPVźCMV
This mode is an active-ventilation mode by volume ventilation (Volume ventilation), meaning A/C.
The taking air quantity of ventilation can be set in 0.1-2.0L(adult), 0.02-0.3L(pediatrics).
In the active-ventilation, PLV or AutoFlow can be chosen.
It is completely handled as the trigger window except the active-ventilation time.
After SW6.0, it is written with CMV(Contineous Mandatory Ventilation).
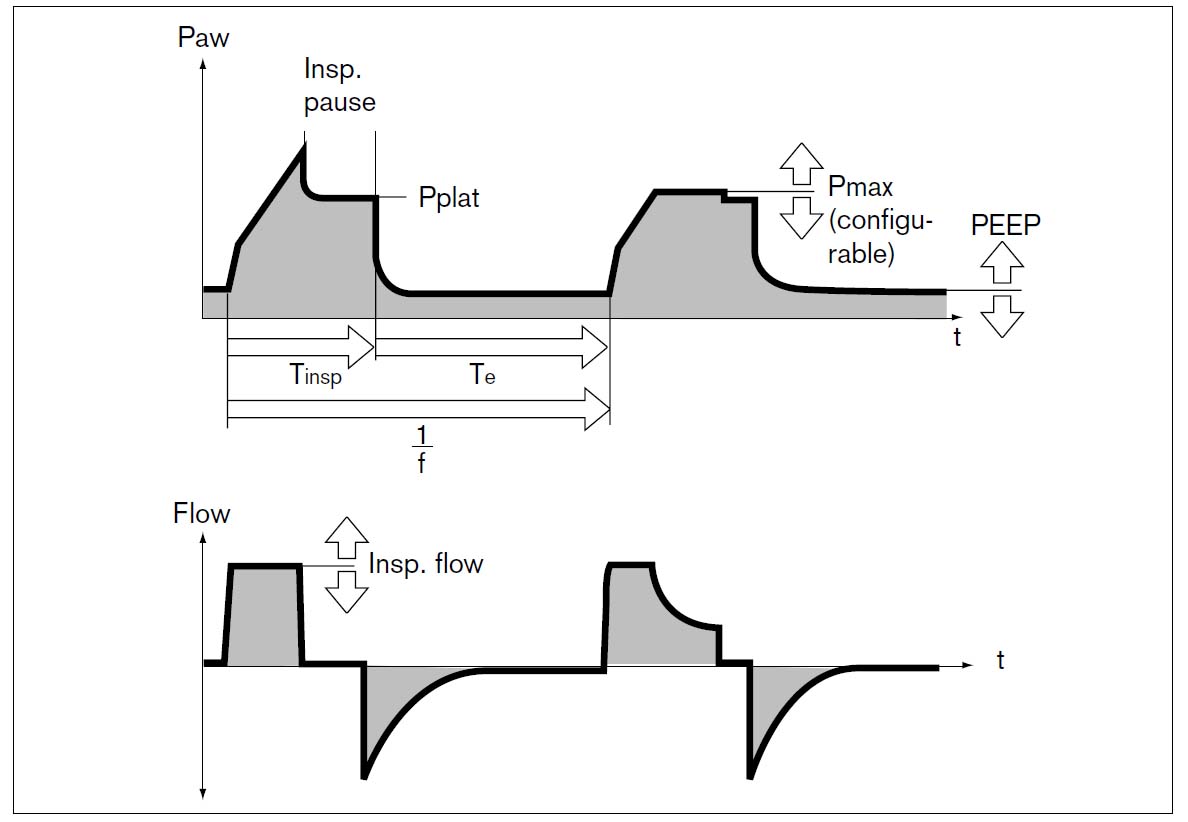
It limits an airway pressure below the maximum airway pressure which was set in "Pmax" in the way of ventilating to make Å]Ś╩ type ventilation "Volume ventilation" and Å]ł│ type ventilation "Pressure ventilation" be compatible.
However, now, the taking air quantity of ventilation doesn't decrease.
It continues intake until it lowers (an = peak shaving) intake flow rate so as not to exceed the pressure and a set taking air quantity of ventilation is stored when the airway pressure reaches "Pmax" like the figure (It becomes PCV of volume cycle).
Now, it is T.EIP(The intake plateau time)
decreases. TEIPBecause "WOKOETE" intake time is never extended, this becomes the limit of the compensation for the air quantity of ventilation.
When an air quantity of ventilation is decreased, it is made "volume not constant" by the message and the warning sound sounds.
Incidentally, the value with +10 mbar of set values becomes the alarm level of the maximum airway pressure automatically.
It is not a ventilation mode but it is the feature which can be added to the IPPV, SIMV, EMMV mode.
It is possible to say to BIPAP which is pressure ventilation that it does the function to guarantee a taking air quantity of ventilation.
The completeness or there is not division in the one to set to the active-ventilation with the front of adding operation with the spontaneous-respiration aspects such as SIMV.
It puts the taking air quantity of ventilation which used to the full in the intake time which was set first, set goal pressure when choosing this feature and was prescribed (The general volume ventilation).
It makes the plateau pressure which occurs at this time initial setting pressure.
Since the 2nd, it sets a ventilating-pressure, calculating from the compliance in the last time and the air quantity of ventilation at the time of the active-ventilation.
It limits a variation within 3 mbar.
The upper limit of the pressure change becomes the -5-mbar value of the pressure upper limit alarm.
Also, the upper limit of the air quantity of ventilation can be set with the "Vti" alarm, too, (It shifts to the low pressure aspect simultaneously with the alarm).
It is possible to say the feature which it is possible to set "having width" for which it is difficult to wake up Fighting by the setting feeling of the conventional Å]Ś╩ type (the volume control) to Å]ł│, too.
Of this mode however, it is possible to adjust increased pressure speed.
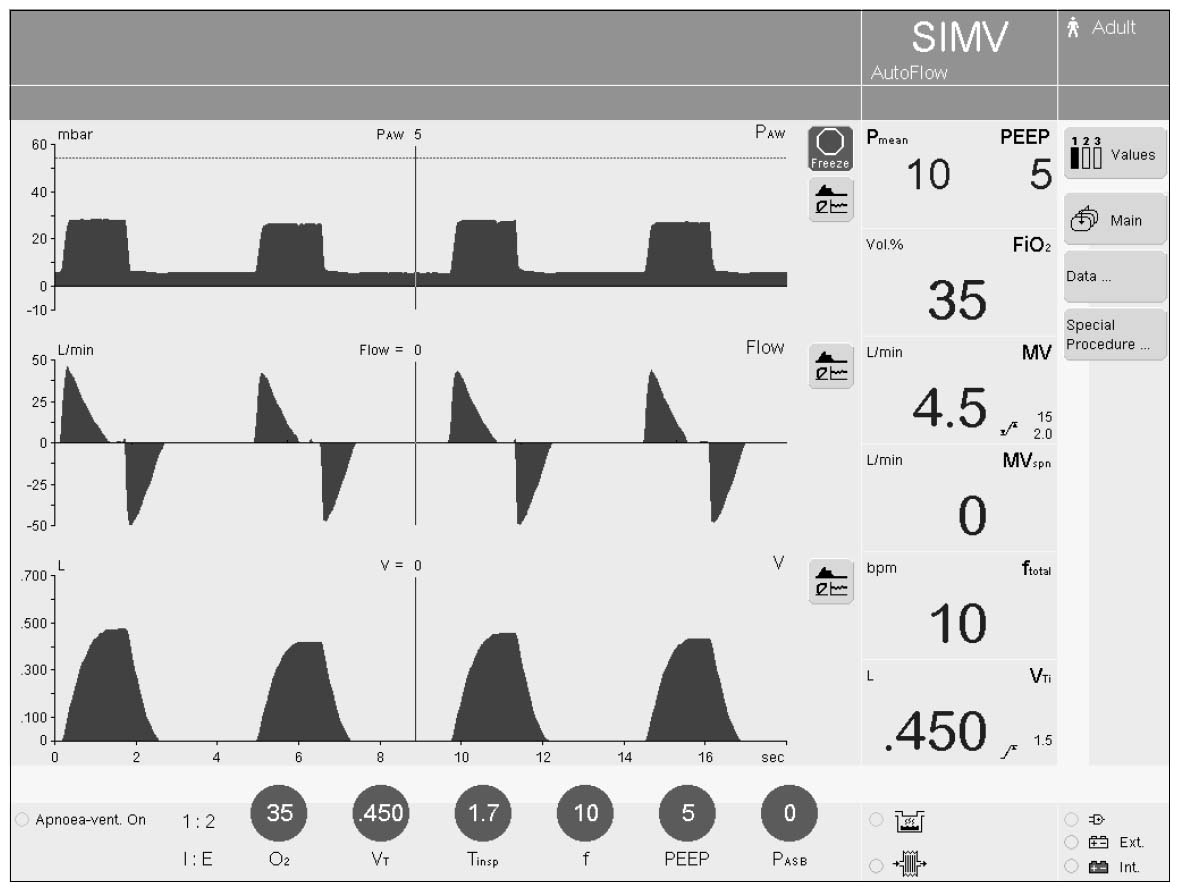
6)SIMV
As for the trigger wind of Evita, by the fixation in 5 seconds, an active-ventilation is done only for the first trigger of the SIMV cycle.
The time of the SIMV cycle with once becomes 5 seconds of 12/60=, i.e. all of the SIMV cycles become a trigger wind when setting SIMV to equal to or more than 12 times.
It does a trigger to done intake for the first time into the SIMV cycle with once, it does an active-ventilation and the time of the remainder becomes a spontaneous-respiration aspect.
When the intake which was begun in front of the following trigger wind continues to the following trigger wind, at the same time as the following trigger wind begins, voluntary intake shifts to the active-ventilation.
But, because the quantity which excluded the capacity which was sucked with voluntary intake from the set taking air quantity of ventilation is supplied as the active-ventilation about the active-ventilation quantity in this case, dangerous surplus intake is evaded.
The active-ventilation number of times doesn't change even if the SIMV number of times active-ventilation to have set to 1 minute in EVT-4000 is done and there is a spontaneous-respiration.
(1 revolution per minute of set value +-)
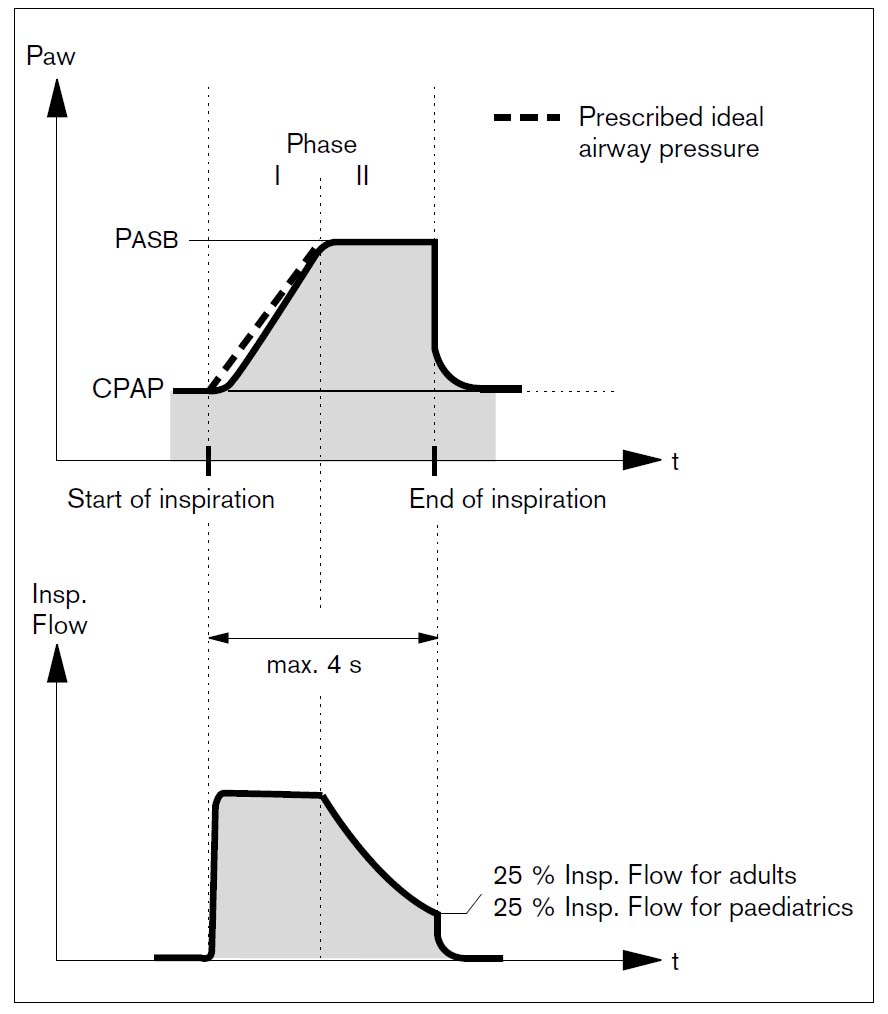
In the Drager Inc., the spontaneous-respiration help mode of the PSV similarity is called ASB.
phase-2 of ASB is phase-1 pressure maintenance period in the pressure start-up period.
It is possible to be expressed by general ASB when it is ASB which becomes phase-2 suddenly.
Because pressure is rapidly gained by the respiratory tract in the high PSV level at the equipment that the maximum supply possible intake gas flow rate is high, it brings about strong pressure and the phenomenon which is against PSV, being reflex, too, is admission "RARU".
ASB is controlling, dividing into phase-1 and phase-2 to solve this. As for phase-1, in the period where there is an increased pressure, the standard pressure rises continuously with the passage of time.
This speed (in other words, are the time of phase-1) is variable in 64ms-the 2.0-s range.
phase At 1, an intake valve is adjusted for the inspiratory-pressure to consist of standard pressure within -0.6 mbar.
If there is an equal to or more than -0.6-mbar difference, the early stage intake gas flow rate becomes 120LPM.
When the inspiratory-pressure exceeds standard pressure, ASB ends and shifts to the expiratory-phase at once.
phase 2 is the step which maintains a set-pressure, but when the intake flow rate declines in 25% (the time of 6%, the infant mode) of the peak rate of flow, it judges and switches over the ending of the inspiratory-phase and a machine to the expiratory-phase.
Incidentally, in the intake time, it is limited to a maximum of 4 s (the time of 1.5 s, the infant mode).
EMMV of the Drager method is similar to the method of Erica, Elvira that it is made by the Engstrom Inc..
(The algorithm that) the intake expired volume per minute which was computed based on the data in 20 seconds of the pasts in Evita (is specific) is Vt, f when falling more than the eye token expired volume per minute which set (a corporate secret).IMVThe SIMV cycle which is starts.
(Order of the trigger wind, the inspiratory-phase, the expiratory-phase)
However, the setting f when becoming "APUNIA" suddenly after the patient expired volumes per minute which are much more than the goal expired volume per minute occurIMV However, when becoming setting with + trigger wind time of 7.5 seconds,-8 onces equal to or more than eight times, an active-ventilation is done behind the SIMV cycle time + trigger wind time with once.
In the trigger wind time, it is a fixation in 5 seconds.
Therefore, in the time that an active-ventilation is begun after the anaerosis occurs actually, it is 12.5 seconds-(60/f.IMV + 5) The second becomes necessary
The heat ray of "HURO-SENSA" on the side of the expiration is broken because EMMV of Evita is controlled by the expired volume per minute on the side of intake and the proofreading doesn't influence the operation of EMMV by being being upset, too.
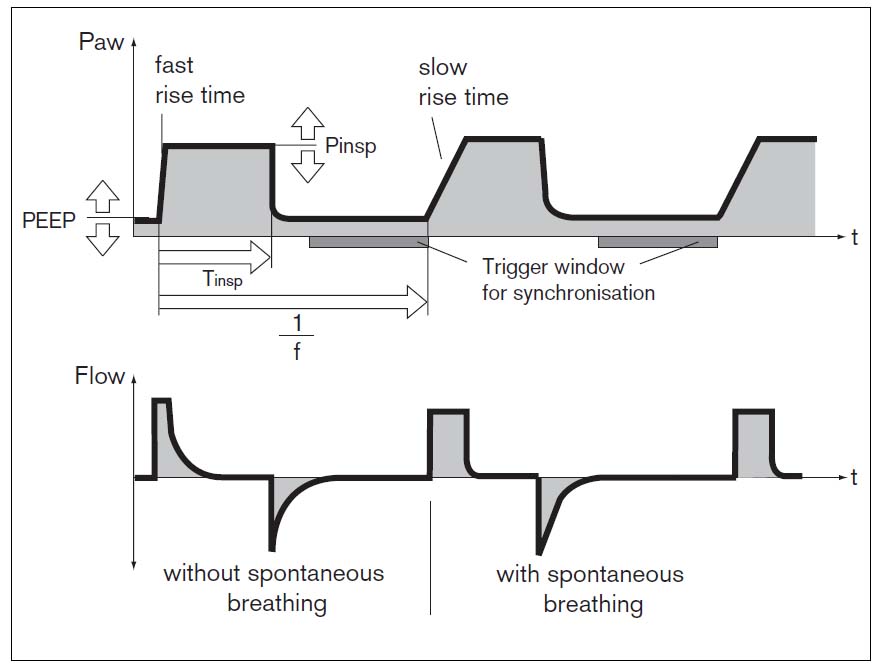
BIPAP which was introduced by Evita was the variation of CPAP at first but after Evita2, it became the general mode to contain a mode of the ventilation of the PCV similarity.
This mode is the optional duration (0.2-60 seconds in case of BIPAP-APRV) which set the pressure (the high-pressure aspect : 0-80 mbar of Pinsp=, the low pressure aspect : 0-35 mbar of CPAP=) of CPAP with two levels and is the ventilation mood which changes alternately and helps breathing.
In BIPAP, the trigger wind opens when the pressure of CPAP switches over to the low pressure ü© high pressure or the high-pressure ü© low pressure, too.
This trigger wind opens from the end of the set duration to 25%, and synchronizes with the spontaneous-respiration and the CPAP level switches over.
Float rigger (0.3-15LPM) is used for the recognition condition of the change from the low pressure aspect to the high-pressure aspect.
The switchover of the low pressure aspect is done from the high-pressure aspect when the intake gas flow rate becomes 0LPM.
In the low pressure aspect, ASB, too, is the multifunction mode to include the concept of ĢŽ¢@ of SIMV(PCV)+PSV-PCV-CPAP because it is possible to use.
Moreover, in addition to having the characteristic that very little overshoots and under shot occur at the pressure corrugation because BIPAP is done by intake and expiration valve both together style operation, it provides ideal pressure ventilation along with that the call worrying, too, operates by the trigger.
Of this mode however, it is possible to adjust increased pressure speed.
Incidentally, there is not a trigger window, in EVT-4000, it doesn't synchronize with the spontaneous-respiration and the pressure switches over to APRV.
ü@
BIPAP assist means the ASSIST mode which is made by BIPAP.
The pressure ventilation which is made with BIPAP to all triggers is provided.
Therefore, the point of whose operating by the BIPAP system by it of being equal to the PCV mode almost by BIPAP assist the intake expiration of what tense of the inspiratory-phase and the expiratory-phase however, is possible is an advantage.
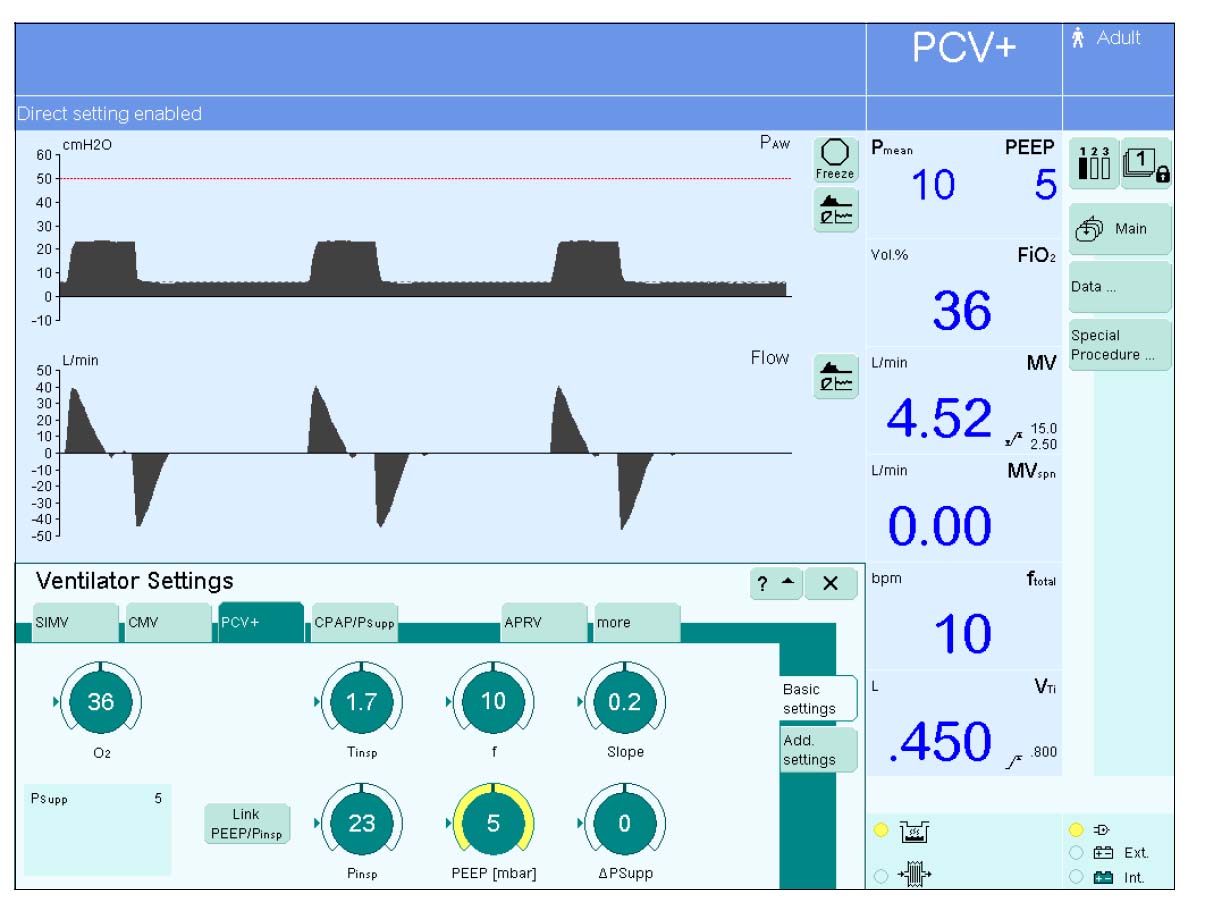
After SW6.0, it is written with PCV +.
Only the IPPV mode is valid.
It hangs SIGH by changing PEEP pressure in Evita.
When thinking of the original purpose to prevent the falling into a state of lethargy of the alveolus, SIGH by the pressure is more logical than SIGH by the volume.
There are few extraordinary rises of the airway pressure in this one.
It prevents the abnormal addition of the pressure along with PLV.
12) Apnea ventilation (The anaerosis back-up)
Because there is a backup mode to the hypoventilation by EMMV, it thinks that the anaerosis back-up feature is unnecessary but moreover, there is anaerosis back-up feature "Apnea ventilation" in Evita.
This feature can be added to the mode except EMMV, IPPV, i.e. each mode of SIMV, BIPAP, APRV, ASB.
When adding this feature, it shifts to the active-ventilation at the same time as sounding an alarm when lasting in the time (it is possible to set within 15-60 seconds) which the anaerosis set.
The taking air quantity of ventilation and breathing number of times in case of this back-up operation can be independently set.
To switch over to the active-ventilation behind the anaerosis resembles "Apnea ventilation" of BENETT-7200ae, in BENETT-7200ae, the IPPV operation returns to the spontaneous-respiration operation, being automatically canceled when detecting a spontaneous-respiration in "Apnea ventilation" but the point which isn't canceled as far as the operator confirms and doesn't push RESET key depends on the Evita series.
Incidentally, anaerosis alarm "Apnea alarm" becomes variable within 15-60 seconds.
(15 seconds of original values)
13) PEEP compensator (The PEEP revision)
The exhalation-valve resistance to expiration gas becomes the factor to change PEEP pressure.
Because the constant pressure gap occurs according to the expiration flow rate in the exhalation-valve, to revise this, as for the exhalation-valve driving-pressure, only the taking advantage of part can decrease an expiration flow rate in 1.9mbar/L/s.
Being general, the flow transducer information of the expiration is for the alarm, but it is possible to hold respectively and is used as the control-information.
14) Leak compensator (The leak revision)
Leak compensating machine Ź\ works and the gas of a maximum of 20 LPM is supplied when there is a leak and PEEP declines from the set value in the IPPV/control mode.
In the IPPV/assist mode, this compensating machine Ź\ doesn't work.
This is because compensating machine Ź\ can not exclude the danger to interfere with the trigger operation by by working.
When the leak occurs in SIMV and the CPAP mode, it works so as not to supply a maximum of 120 LPM gases like voluntary intake and for the pressure of PEEP and CPAP to fall.
15) ILV (The either side lung independence ventilation)
A connector for ILV(Independent lung ventilation) to work two Evita by making them synchronize electrically is attached.
16) The output
It is average and the digital output by the RS-232C is possible.
The PC monitor can be used by doing him like the slave monitor of Evita when connecting the Windows PC to have incorporated the Ebita view of the option into.
The airway pressure, the intake expiration gas flow rate, the analog output about the item of the air quantity of ventilation, too, are possible if incorporating the Ebita 4 link of (the display of the corrugation and the trend) and also the option.
Incidentally, it is SpO which is prepared as the option.2Breathing and the circulation can be evaluated at the same time in the measurement if
incorporating a measurement kit. But, it is SpO recently at the electrocardiogram monitor.2However, because there are many cases which are incorporated, being average, it may not need this.
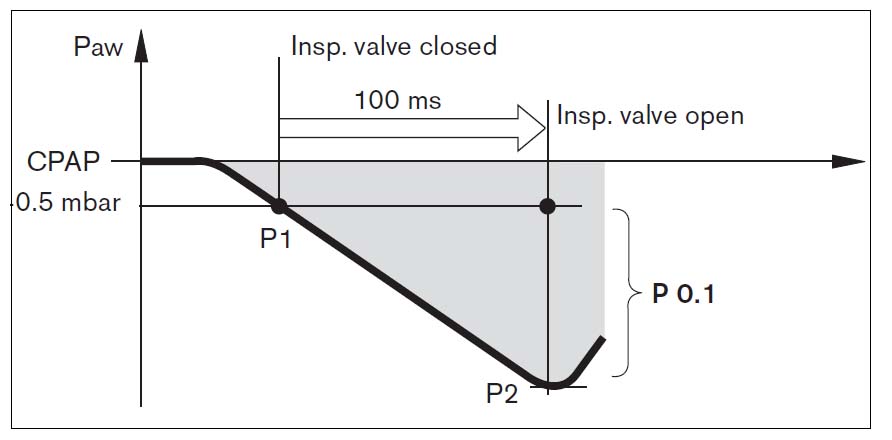
17) The Intrinsic PEEP measurement
The trap volume the pressure of Intrinsic PEEP (PEEP which is caused by the internal cause) OBJ DO and of which an exhalation-valve intake valve is to that twined by closing it in case of the expiration end can be measured.
After intake beginning is recognized, it is P in the negative pressure in the respiratory tract behind 100msec.0.1 It is called ("WAN" pea
point). P0.1Among 100msec, it consists of the intake beginning which was recognized after pushing a
beginning key with the blockade period when the exhalation-valve and the intake valve are
closed. P0.1It is the index of the power level of the "HA" respiratory center and it is used for the estimate of the weaning success or failure from the resuscitator.
19) The nebulizer
Because it adjusts an oxygen concentration by the switching of the Y1.1 valve, depending on the setting, the error occurs in the oxygen concentration.
The error occurs with the expired volume per minute and the oxygen concentration when not using a special nebulizer.
Because it isn't possible to finish compensating for the error of the air quantity of ventilation and the oxygen concentration in the mouth by nebulizer drive gas when set to the low flow rate below intake flow rate 15LPM and changing to the infant mode, automatically, a nebulizer is OFFd.
20) The battery backup
In case of power blocking-off, it is possible to operate for equal to or more than 10 minutes by the inner battery.
21)ATC(Automatic Tube Compensation)
ATC is the processing which does the airway resistance of the tracheal tube in the compensation, being called electric decannulation Electronic extubation, too.
It said that PSV of 3cmH2O did the resistance of the patient circuit empirically in the compensation but actually, the pressure inclination which is proportional to the gas flow rate of the respiratory tract was occurring.
It is the translation in the simplicity 3cmH2O PSV OBJ DO, and to be equal and to have been expressing an average with this pressure inclination.
The mechanism to pressurize by beforehand adding the pressure inclination which occurs with the gas flow rate is ATC.
ATC can be added to the mode of all ventilation.
If changing a viewpoint, it is the mechanism to shoulder the part of the airway resistance to help in Flow gain in PAV which is explained at the following item.
To use this feature, it pushes Tube Comp. key and it chooses On and it chooses ET Tube (the tracheal-intubation tube) or Trach. Tube (the tracheostomy-tube).
Next, it enters a tube size, Comp. (the degree which is in the compensation, 0-100%).
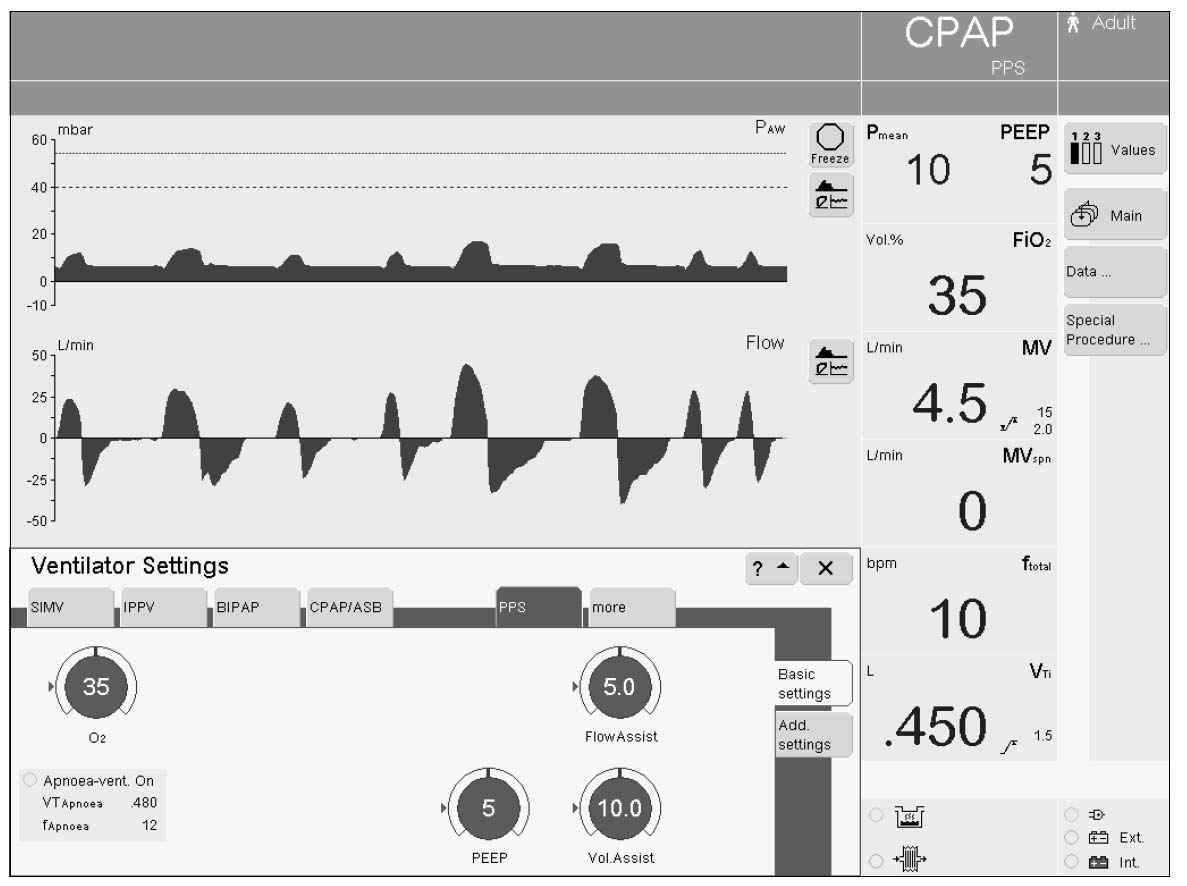
PPS is the PAV one.
The Drager Inc. has the cacoethes which uses a unique term for the mode name but this, too, is the same.
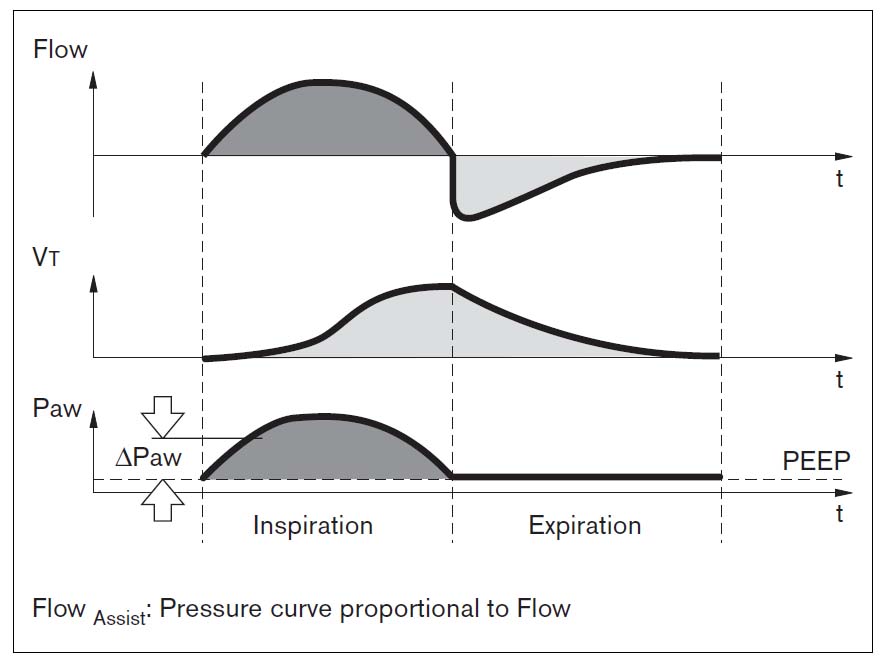
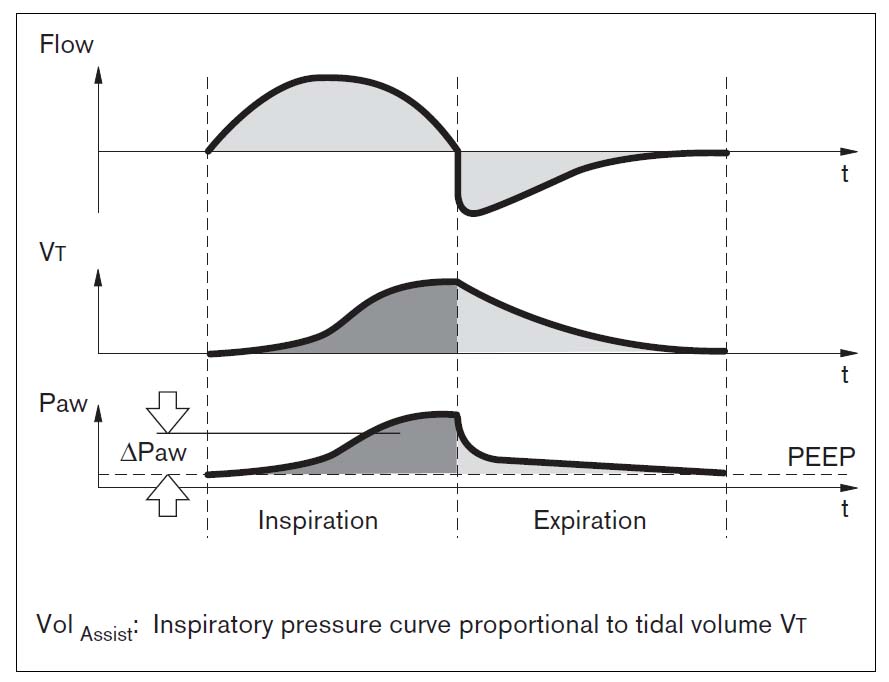
PPS must set two gains of Flow Assist (
figure ; explanation of Flow Assist) and Volume Assist (
figure ; explanation of Volume Assist).
To measure these optimum gains, it is explaining that it is handy to use Runaway phenomenon.
The Runaway phenomenon occurs when raising these gains.
The Volume high alarm and the airway pressure upper limit alarm operate continuously now and
As for the patient who draws a curve which descends immediately after that with the flow curve reaching the upper limit suddenly, (Flow Assist) which causes an auto trigger to do the air of the lung that an over-expansion is consciously done using the expiratory-muscle in the summon, "NADOGA" causes to try do are observed.
It is said to that 80% of gains ahead by one step which causes Runaway phenomenon are an optimum gain.
22)NeoFlow
The adaptation of Evita is equal to or more than 3-Kg weight but equal to or more than 3-ml PTV becomes possible in the 500-g weight, the taking air quantity of ventilation when equipped with NeoFlow of the option.
In NeoFlow, the continuous flow of 6LPM is flowing in the expiratory-phase.
Because a thing for the setting and the demand is supplied from the intake valve in addition to the continuous flow of 6LPM in the inspiratory-phase, it doesn't become extinct and the gas of 6LPM flows through the exhalation-valve regardless of intake and the expiration.
Therefore, even if it doesn't put on with the simile trigger in NeoFlow, as for breathing work volume, are the least.
It is controlling an inspiratory-pressure in relieving a continuous flow in the pressure by the exhalation-valve in BabyLog8000 which is the newborn baby personal plane of the company, but Evita advances by one step and is controlling an inspiratory-pressure in the balance of the exquisiteness of the intake valve and the expiration valve.
Therefore, the ironhand ability was high and of correct ł│ɦīõ which doesn't have an overshoot and an under shot however, it became possible.
Fluothane Sir uses the one of BabyLog8000 and attaches an interface board to the slot of the back newly.
That NeoFlow can use all artificial respiration modes such as ATC and PPS in addition to BIPAP and AutoFlow, MMV is the characteristic which should mention specially.
As for another characteristic of NeoFlow, even if there is a leak from the cuff pear trachea tube, the trigger sensitivity is the things which are few in the malfunction by the leak because it is that a leak is revised.
Therefore, it considers an amount of leak and to make trigger sensitivity low isn't necessary.
For example, 0.25LPM is realistically recommended because the best trigger sensitivity of Servo i is 0.05LPM but there is not leak revision.
In other words, it is equal to 0.3LPM of Evita.
Leak revision by Evita is based on the following theory.
The difference between the intake expired volume per minute and the expiration expired volume per minute is an amount of leak but it supposes that the amount of leak is proportional to the airway pressure.
Because the amount of leak in the past is continuously measured, it can expect an amount of leak according to the airway pressure.
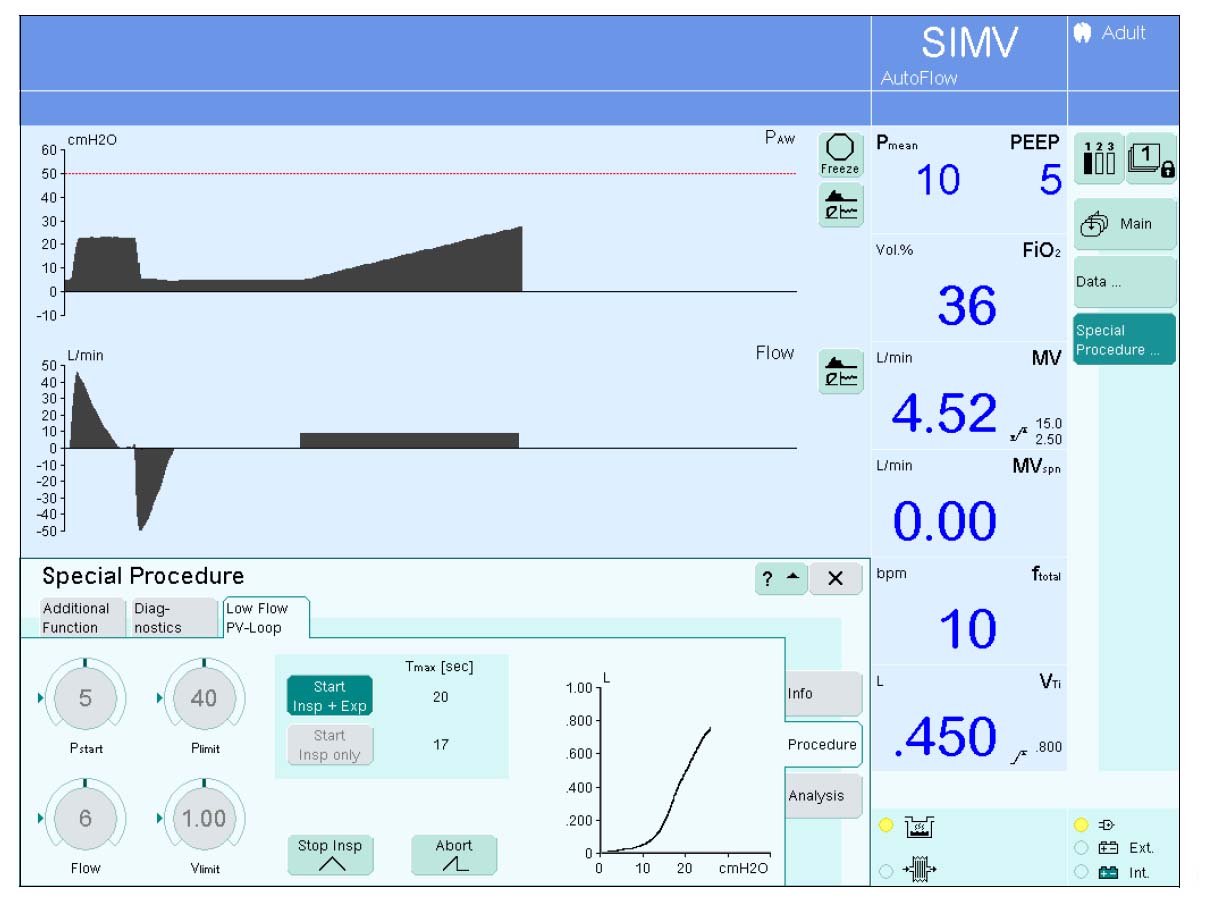
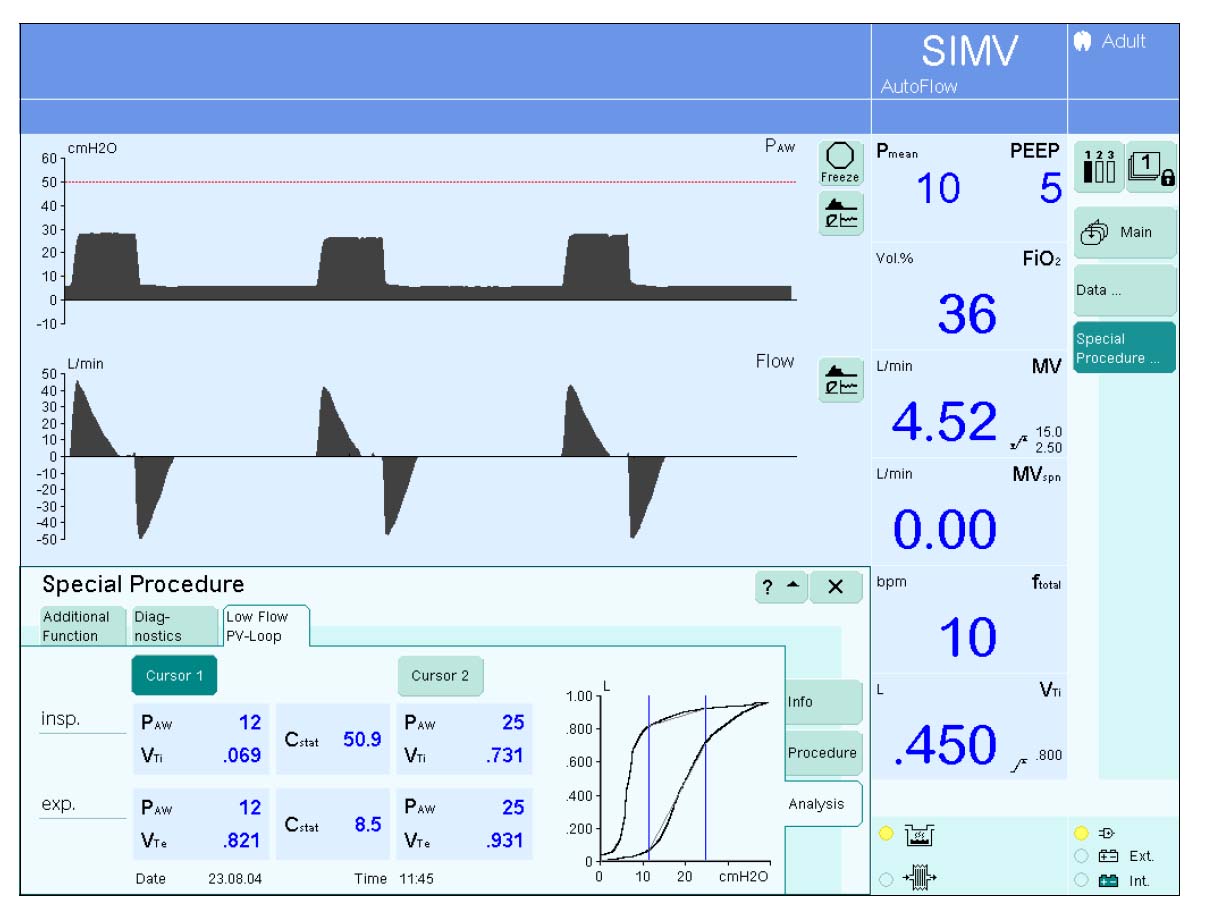
It is possible to use in EvitaXL. It is the feature to measure
PV loop correctly.
24)SmartCare
It is the function to do the ventilating-pressure of PSV in the self-regulation to maintain a comfortable condition (called a comfort zone) for the patient and to wean automatically.
The infant with 15-35-Kg weight and the adult with equal to or more than 35-Kg weight are an object.
The adult can use ATC, too.
The operation is rather different HME or heating humidifier, COPD existence or non-existence, central nerve fault existence or non-existence, boiling therefore.
It puts on weaning in night, too, in ON/OFF.
ü@
The infant comfort zone is
hereinafter.
Breathing number of times :
18-40 bpm
The taking air quantity of
ventilation : 6 ml/KG BW
CO2 :55 The following of
mmHG
It is 10 mbar to the PS goal
pressure=all the patients.
ü@
The comfort zone of the adult is hereinafter.
Breathing number of times : 15-30 bpm (Being 34 in case of doing
central nerve fault attractive and in the case To bpm)
The taking air quantity of ventilation : 300 ml
equal to or more than (BW < 55 KG is 250 ml)
CO2 : 55 The following of mmHG (To 65mmHG in case
of COPD)
Maximum breathing number of times=36 bpm
(The serious tachypn ea)
The PS goal pressure=5 (The heating
humidifier and the tracheostomy)
The PS goal pressure=7 (The heating
humidifier and the
tracheal-intubation)
The PS goal pressure=9 (The
artificial-nose and the
tracheostomy)
The PS goal pressure=12 (The
artificial-nose and the
tracheal-intubation)
ü@
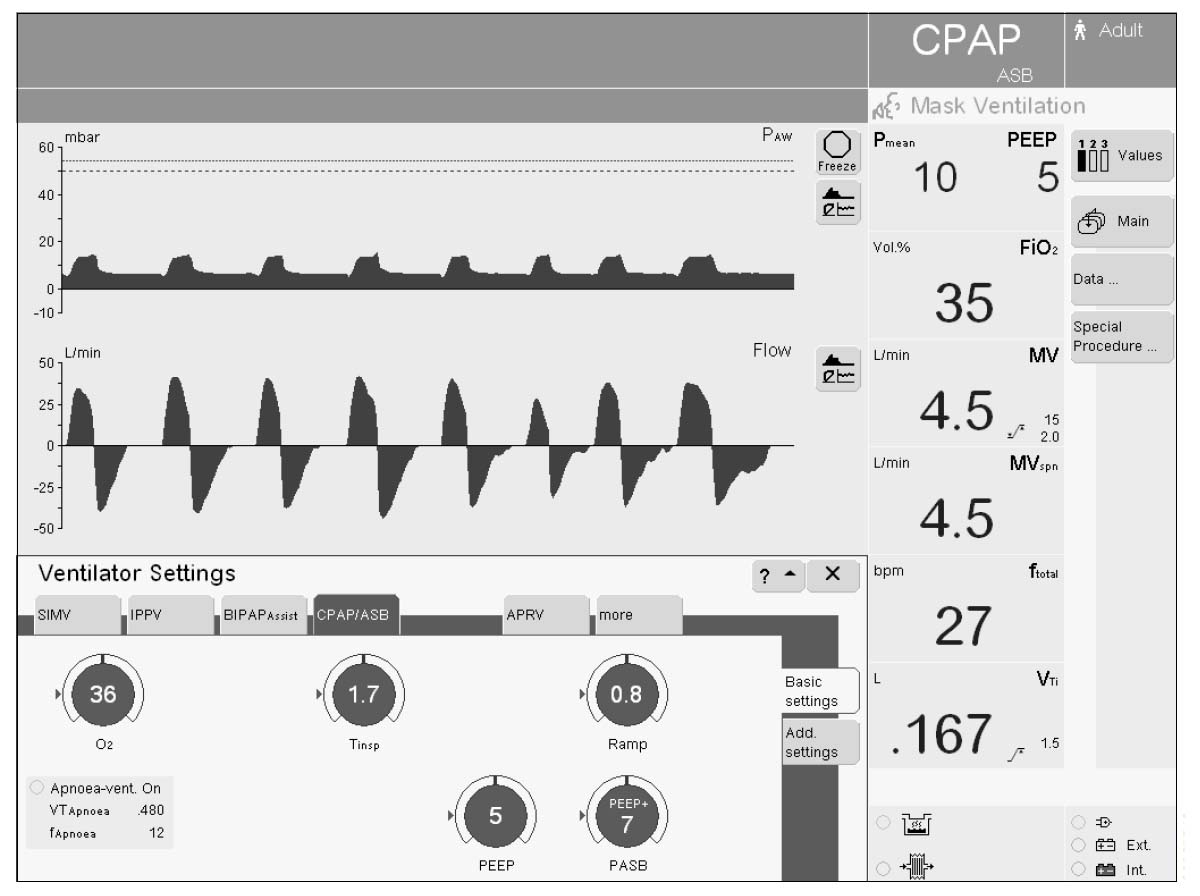
It is a mode for NIV to ventilate under the mask. There is an oxygen inhalation mode which
operates as ordinary oxygen supply, too.
1) The basic operation
The large-sized touch panel system TFT display can set visually.
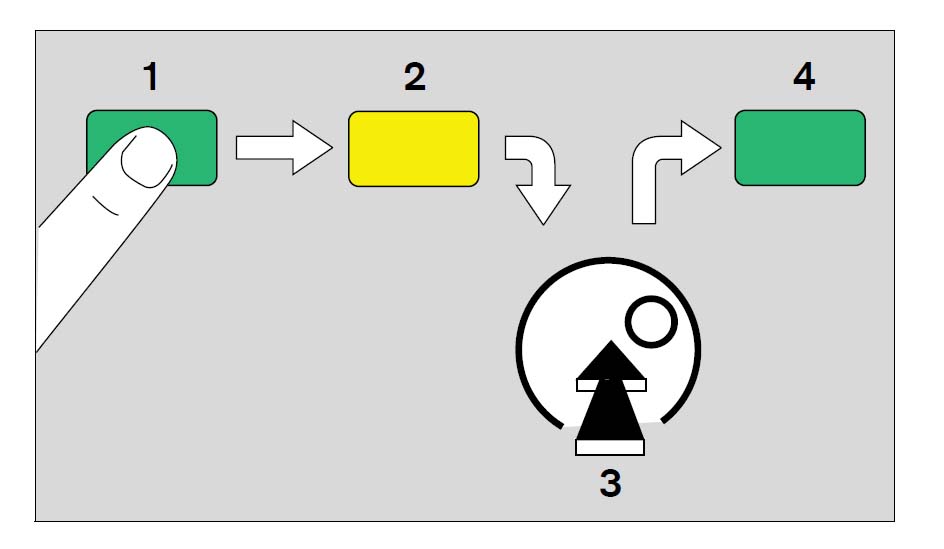
The basics of the setting push the ćB rotary knob which turns a screen knob with the item which sets ć@ and the ćA rotary knob which touches a key and it fixes an input value.
It is a setting method having to do with a mouse.
The operation of being fixed is necessary every item.
Because it isn't possible to change actually even if it switches over to the other item without being fixed, a confused case is occasionally seen.
(It is "HO-MUPE-ZI").
The most basic screen is a ventilation mode setting screen.
This is displayed when it pushes "the ventilation mode setting" key in the right of the electrochromatic display screen.
In this screen, in the top, with the graphic corrugation (Flow, Press, Volume can be chosen), the lower-half is the setting screen of the control.
Because it puts on 4 optional items (for example, are the actual measurement of Vt, f, the MV, EtCO2), too, by the numeral display, most case is enough in this screen.
As for the setting items such as the taking air quantity of ventilation, the oxygen concentration, breathing number of times, according to the chosen ventilation mode, a control is discovered only about the necessary item.
It is displayed by the triangle that the standard of the setting by the weight is Midori more.
When setting intake time, the small window screen appears and displays I:E ratio specially.
It displays an operation guide in most screen Shitadan when pushing i key (the information key).
3) The alarm setting
Next, it is the alarm setting screen that is important.
This screen is displayed when it pushes the button of the alarm setting of the right of the electrochromatic display screen.
Because a customized value is stored in the original value about the upper limit, the minimum, to readjust most item should not be necessary.
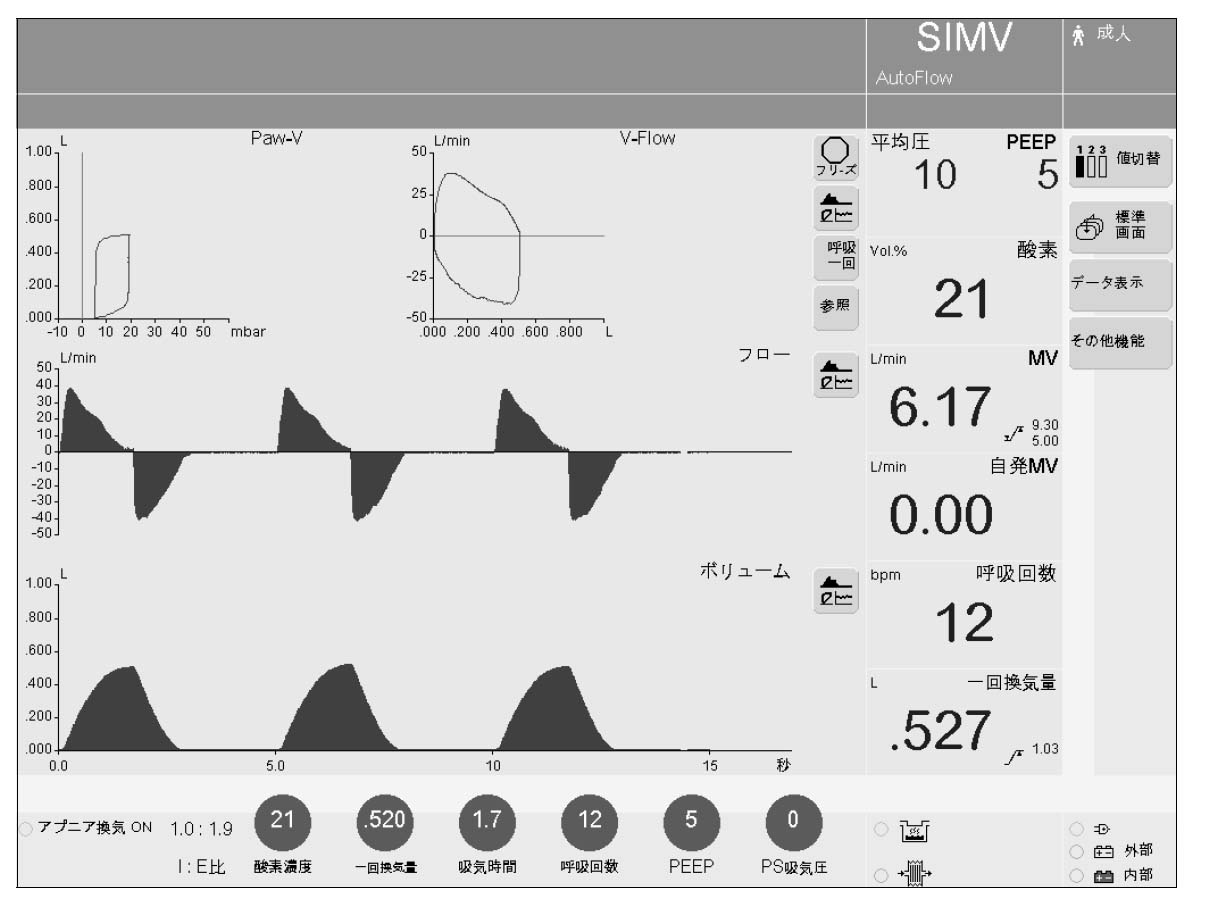
It is displayed when pushing a screen-display reversing key. Two kinds of optional corrugations can
be displayed. As for the scale, there is automatic setting.
5) The measure
The measure (the value), the various mechanics screen, Log Book can be displayed when pushing this key.
6)EMMV
The goal expired volume per minute of EMMV is a taking air quantity of ventilation and f.IMV It is established in the product which is.
The small window screen appears and displays the calculated value of the product specially.
Because it often becomes an item with the goal expired volume per minute which was independent at the other equipment, at this point, note is necessary.
7) The special function
The basic feature can set in the background information even if it is not, the first setup (the customize by the user) may be complex but it is possible to be comfortably used by it when setting once.
It requires a password entry so as not for the item to be able to change carelessly.
The setting range of the alarm, too, is automatically set to the environment operating but this original value, too, can be changed, too.
The original value of the corrugated kind, the combination of the numerical data to make always display, the combination of the mode key, the corrugated combination of the trend and so on can be changed into the others, too.
Pressure unit mBar, mmH2O, too, can be chosen.
When not changing, a manufacturer original value is chosen.
8) The customize of the screen
The beginning screen (the initial-screen) when turning on can be customized.
ć@ The way of beginning to set weight (In Drager, it is called Ideal body waight).
ćA The adult or the infant, the way, the "WOARA" rudder eyes that the set value which is peculiar to each begins can be chosen.
There is a alternative of the growing up, the way of beginning that the infant can be chosen, the way of beginning by either of the adult or the infant mode the fixation in ćA more.
For example, the weak point is in the fixation mode for the adult when chosen and is the case which must be rarely started by the infant business.
In this case, the labor which restarts after changing a customize screen is necessary.
It hopes as it is possible to jump to the setting screen by Ideal body waight.
7. The monitor, the alarm
function
Automatic setting is made the following condition if the patient relation does necessary setting.
It sets only an expired volume per minute with the manual.
1) The oxygen concentration
When the equal to or more than 4-vol% difference occurs between the set value and the actual measurement in case of equal to or less than 60 vol% of set values
In case of equal to or more than 60 vol% of set values, the alarm that the equal to or more than 6-vol% difference occurred between the set value and the actual measurement occurs.
2) The airway pressure
When becoming above the value which was set with the Paw ceiling-value of the alarm setting screen
It sounds a low pressure alarm when the peak value of above 96msec doesn't cross +5 mbar of PEEP of 2 breathing continuously even if it does an active-ventilation.
3) The expiration expired volume per minute
When deviating from the set upper limit, the minimum
4) The anaerosis
When second number (15-60 seconds, 15 seconds of original values) set equal to or more than breathing stops
5) Equipment's being mal-function
The oxyecoia-supply, the compressed air supply, the O2/ It does abnormality of the AIR burner-mixing-tube, the pressure measurement, the fan, "HURO-SENSA", the exhalation-valve unit, the O2 sensor, the temperature sensor, the power, the inner electronic circuit, the inner "NIYU-MATITUKU" circuit in the caution.
Also, it does a caution even if it opens a patient circuit. In this case, it should
open after pushing 100%O2 key.
In Evita4, it displays two kinds of corrugated graphs. This corrugation is an airway
pressure, a flow rate corrugation, a flow rate corrugation, CO.2 Two corrugations can be displayed by choosing while being a pulse wave form when incorporating a corrugation (the option).
In addition to four measured value displays that a normal video is done, it is a setting control, a trend graph.
It is SpO with the loop corrugation, the list display of the measure, the operation in the past, the list (the logbook), the special measurement display of the alarm record, the reading in the corrugated halting and the digital of the value of the stopping corrugated data and also the option.2It is possible to do the display of the digital data which is.
Menu screen such as the device check when doing special operation, too, spreads out respectively.
When making a flow rate corrugation, in the SIMV mode and so on, it does corrugated classification by the active-ventilation and the spontaneous-respiration and it makes it easy to grasp breathing status of the patient.
The trend graph of the expired volume per minute, too, is same.
Because it is possible to use as the graphic display which is corrugated in 3 when incorporating the software which is called Evita View into the cheap Windows laptop computer, it is convenient when getting ready beforehand.
In EvitaXL, it is average and the various display is possible.
9. The patient circuit composition, the
humidifier
When the heating humidifier (Fisher & pie Kel MR-410) infant of "DEISUPO" type and the it thermal management must be made precise, inside the heating humidifier (Fisher & pie Kel MR-730, MR-850) with the heater can be chosen from.
10. The maintenance
1) The proofreading of a sensor
In Evita, it is a lot of pressure sensors and "HURO-SENSA", temperature sensors, O.2 A sensor is used. An auto-calibration is continuously done about the pressure
sensor and the temperature sensor. Also, it is O.2 It is made the back of the taking late-morning on the 1st by the
auto-calibration about the sensor and expiration "HURO-SENSA", too. The
O2 The sensor, and expiration "HURO-SENSA", CO2 Therefore as occasion demands now in the sensor
It is possible to proofread when an alarm is sounded when exchanging a sensor and the question is in the precision.
It is possible that to unbuckle a circuit from the patient by each sensor isn't necessary and to proofread it anytime.
" It chooses the sensor to want to proofread by pushing a proofreading " key and it presses a key only.
Because the circuit which prevents proofreading gas's flowing through the patient to be used for the O2 sensor by the infant that the rise of a few oxygen concentrations, too, becomes dangerous therefore, too, is had, the proofreading can be implemented without having an influence on the patient (About 1 minute).
2) The exhalation-valve
The exhalation-valve becomes a removable type unit and removes unit "TO" and washes pouring with the tap water.
Therefore, in the ordinary use, the labor of the resolution wash is unnecessary.
It dries up in the sterilization with the autoclave after wash.
This exhalation-valve unit was much light-weight more than EVT-1000 and became cheap.
It makes sparely, being sterilized and two exhalation-valve units in amount are attached to the main unit.
Incidentally, the example which was made a malfunction with a continuous running duty there being without washing for about 1 year is reported.
3) The flownmeter on the side of the expiration
It is impossible for this "HURO-SENSA" to be sterilized because the heat is linear.
Therefore, it becomes "DEISUPO" and assume that it exchanges every patient.
Physically, the continuous running duty, too, is possible.
4) The O2 sensor
This needs an exchange when consuming because it is moth Le Bas Nick cell "galbanic cell".
11. The regular
inspection
It is necessary to check by the technical service every 6 months.
12. The
fault
1) The mode which Evita4 can choose on the setting screen is only four kinds.
To choose the mode not to be displayed, the procedure which restarts after changing an initial setting screen is necessary and is very inconvenient.
This was improved in EvitaXL.
2) There is danger which forces into the ventilation effort which is unnecessary for the patient in AutoFlow if there are too much few setting taking air quantities of ventilation in it to the air quantity of ventilation which the patient demands.
There is possibility that it is possible to prevent this if the least ventilating-pressure can be set.
3) It is only 2 corrugations that it puts on by the simultaneous display to the graphic display.
This solves if it installs VentView in the laptop computer and uses it as the slave monitor.
It was improved in EvitaXL at this point, too.
4) When using a nebulizer, the oxygen concentration is the biggest and causes an error within 4% of +-. Also, in
the low flow rate setting, the nebulizer can not be used.
5) There is Fluothane Sir in the Y peace in NeoFlow (the newborn baby mode), the small patient circuit to be necessary has the load having to do with weight and it is negative.
Only as for this Fluothane Sir, not to work neatly, too, is inconvenient if not proofreading by the manual operation.
6) The best trigger sensitivity in case of NeoFlow is 0.2LPM in 0.3LPM, EvitaXL in Evita4 but it isn't enough for 0.05LPM of Servo i in the thing like a figure when comparing.
But, because there is not leak revision in the trigger sensitivity, the manufacturer is equal to Servo i realistically because it is recommended to use by the sensitivity with degree as 0.25LPM.
7) Isn't done the small being of equal to or more than 1 digit of sampling number of times with pressure compared with Servo i.
The adult doesn't notice a problem at all but at this point, in case of NeoFlow operation, when the taking air quantity of ventilation does extreme setting such as 5 ml, air changes per hour 100BPM, the show of the graphic-screen becomes rough.
Of course, this should become the delay and the ironhand "NO" delay of the trigger by the nano-domain.
8) By the BIPAP system, the exhalation-valve participates actively in the ironhand resemblance and it relieves surplus pressure immediately.
Even if the overshoot and the under shot do Fighting without most, the corrugated beauty with pressure that there is not a change in the inspiratory-pressure corrugation, and so on, overwhelms the other resuscitator.
But, "GIYU-TU" and it becomes and it is fun "ZAME" that the unpleasant sound does when relieving in the pressure from the exhalation-valve.
9) The problem of the bug, the problem on the mechanism or the incomplete problem of the maintenance of the user is unclear but there are not few frequencies with the trouble which happens around the exhalation-valve (including Fluothane Sir) (Fluothane Sir's abnormality and PEEP don't reach a set value and there are many leaks by the exhalation-valve in case of intake, and so on).
Only that there is advanced exhalation-valve control technique specially is dear in the boiling, at this point.
10) It is wonderful that the start-up way and the setting, and so on, can be customized.
Automatic setting is done about the alarm, too, but that this, too, can be customized is convenient.
But, because there are few expired volume per minute upper limits, air changes per hour upper limits, taking air quantity of ventilation upper limits, range by which the "NADOHA" customize can be set, that the range must be expanded with the manual after start-up is inconvenient.
11) When the SIMV trigger window begins in being ventilating in PSV in SIMV, it switches over in the active-ventilation from station on the way but only now, the intake time extends from the set value.
Also, the intake corrugation becomes unnatural.
12) Flow Termination % is wished to be made to be able to be set by the user in PSV and PCV, AutoFlow.
but but are not a popular setting screen, of course, are a story in the Extra Setting screen
13) The convenience when working in the suction using the suction button but when working, there was a case to make "HIARI", not resuming automatically when there are many leaks in the patient circuit in the feature that intake gas does an auto-stop for 3 minutes.
The nurse became a form of panic because the machine didn't run.
It should make some message sound during auto-stop.
14) It isn't possible to say that the regular inspection fee is inexpensive.
15) The option of SmartCare and the Low Flow PV Loop measuring function is too expensive. It
doesn't seem a feature as much as it.
ü@
Evita 2 Dura(EVT-2200)
Evita 2 Dura is Evita In 4 less versions, it becomes inexpensive, to be few.
Basically, it is Evita The mechanism which is the same as 4 is adopted.
It adopts a black and white liquid crystal display for the cost reduction, and it does a monitor feature (CO2, the loop, the trend, the logbook, P 0.1, intrinsic PEEP, SpO2) and an analog output (the Ebita 4 link) in the option handling boiling and it omits them.
An operating panel, too, is rather changed.
However, the performance is Evita Being the same as 4, it is equipped with NeoFlow and AutoFlow, BIPAP, APRV, too, of course.
In the range which does ordinary use in this way, it is Evita 4 and Evita 2 There is not an actual difference in Dura.
The main items such as the taking air quantity of ventilation and the oxygen concentration push the item button which is provided onto the operating panel and choose an item and the value types in with the dial.
It pushes a dial last and it fixes value.
The special item types in using the function key and the dial according to the menu which is displayed in liquid crystal.
ü@
Evita 2 (EVT-2000)
EVT-2000 is the revised version of EVT-1000.
BIPAP developed into the pressure ventilation mode that there is a generality from ĢŽ¢@ of CPAP (It changed from narrow sense BIPAP into BIPAP of the wide sense).
It occurred in the upper class of the menu structure and the setting became easier to that in the accompanying, BIPAP.
Also, it lost an overlap by the control and it improved in the operability.
Moreover, it simplifies an exhalation-valve block more and it is improving maintenance.
Ebita's basic performance is common and the high efficiency, the hi-reliability, the sensitive trigger performance and the high maximum intake gas flow rate and so on have a characteristic.
That it is possible to support more to the infant area (the 3-kg weight) than the adult is the same as EVT-4000.
The point which doesn't have AutoFlow to be current has the biggest difference in case of practical use with EVT-4000.
The difference is admitted by the difference (only the small black and white liquid crystal display) of the display ability, the setting method of which the control resembles and it depends, the point which the maximum intake flow is rather inferior to, too, but EVT-2000 however, because it is equal almost like a performance, when considering price difference, in the general use, it may be enough.
However, there is a difference in the extensity in future.
(In EVT-4000, it is PAV mode and Babylog The newborn baby feature, equal "GA" which exceeds 8000 are planned).
It is possible to do connection with the PC and the measurement, the corrugated display of CO2 and so on, too.
1) The basics
First, it chooses a mode.
Then, the LED which displays the item which needs setting every mode lights up.
It should operate the control that the LED lights up.
EVT-1000 had a sharing control but in EVT-2000, the sharing control passed away.
Because the basic setting items such as the taking air quantity of ventilation, the oxygen concentration, breathing number of times are installed in the control of the panel, they set analog-ly.
3)MMV
The goal expired volume per minute of MMV is set in the product between the taking air quantity of ventilation and fIMV.
Because it often becomes an item with the goal expired volume per minute which was independent at the other equipment, at this point, note is necessary.
3)4) The special function
It is possible to set even if there is not background information in the basic feature but usual operation and another operation type are prepared to the change of the adult infant in BIPAP-APRV, BIPAP-SIMV, MMV, anaerosis back-up, ILV, the hyperventilation monitor, ASB trigger sensitivity setting or after the turning on.
In these features, to do a choice or a setting change, it sets the item to hope for, pushing Menu screen which is displayed on the liquid crystal panel surface.
For example, to set a hyperventilation monitor, the complex key operation becomes need.
The user who uses such a feature is thought of as having an appropriate expert knowledge.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}